

Preoperative Nomogram and Risk Calculator for Postoperative Hypoxemia and Related Clinical Outcomes Following Stanford Type A Acute Aortic Dissection Surgery
- PMID: 35548419
- PMCID: PMC9082545
- DOI: 10.3389/fcvm.2022.851447
Preoperative Nomogram and Risk Calculator for Postoperative Hypoxemia and Related Clinical Outcomes Following Stanford Type A Acute Aortic Dissection Surgery
Abstract
Background: Hypoxemia is a common complication after Stanford type A acute aortic dissection surgery (AADS), however, few studies about hypoxemia after AADS exist. The aims of this study were to identify independent risk factors for hypoxemia after AADS and to clarify its association with clinical outcomes.
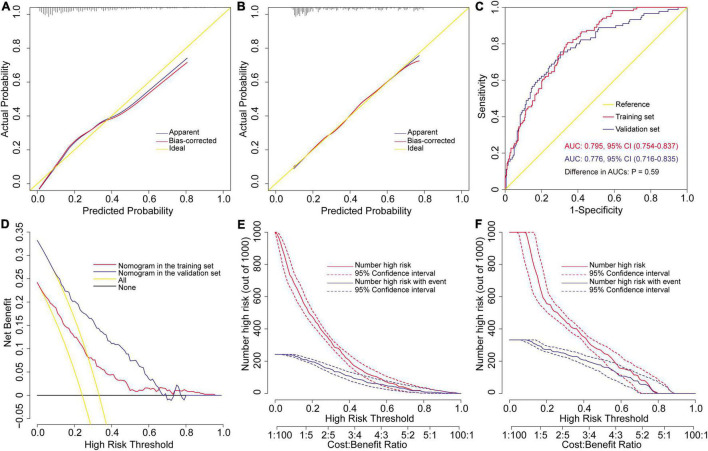
Methods: Patients undergoing AADS from 2016 to 2019 in our hospital were identified and used as a training set. Preoperative variables were first screened by univariate analysis and then entered into a multivariate logistic regression analysis to identify independent risk factors. A nomogram and an online risk calculator were constructed based on the logistic model to facilitate clinical practice and was externally validated in an independent dataset.
Results: Severe hypoxemia developed in 119 of the 492 included patients (24.2%) and poorer clinical outcomes were observed in these patients. Five independent risk factors for severe hypoxemia after AADS were identified by multivariate analysis, including older age, smoking history, renal insufficiency, higher body mass index, and white blood cell count. The model showed good calibration, discrimination, and clinical utility in the training set, and was well validated in the validation set. Risk stratification was performed and three risk groups were defined as low, medium, and high risk groups. Hypertension was identified as an independent risk factor for moderate hypoxemia besides the five predictors mentioned above, and renal insufficiency was not significant for mild hypoxemia by multivariate analysis. In addition, although frozen elephant trunk was associated with increased risk of postoperative hypoxemia in the univariate analysis, frozen elephant trunk was also not identified as an independent risk factor for postoperative hypoxemia in the multivariate analysis.
Conclusion: Hypoxemia was frequent following AADS, related to poorer clinical outcomes. Predictors were identified and a nomogram as well as an online risk calculator predicting severe hypoxemia after AADS was developed and validated, which may be helpful for risk estimation and perioperative management.
Keywords: Stanford type A aortic dissection; hypoxemia; nomogram; prediction model; risk factor.
Copyright © 2022 Sheng, Le, Song, Du, Wu, Tang, Wang, Chen, Wang, Luo, Li, Xia, Huang, Ye, Wu, Du and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources