

Echocardiographic Normal Reference Ranges for Non-invasive Myocardial Work Parameters in Pediatric Age: Results From an International Multi-Center Study
- PMID: 35548421
- PMCID: PMC9081714
- DOI: 10.3389/fcvm.2022.792622
Echocardiographic Normal Reference Ranges for Non-invasive Myocardial Work Parameters in Pediatric Age: Results From an International Multi-Center Study
Abstract
Aims: This international multi-center study aimed to demonstrate the feasibility and reliability of non-invasive myocardial work (MW) parameters in the pediatric population, and to provide normal reference ranges for this useful echocardiographic tool in this specific subset of patients.
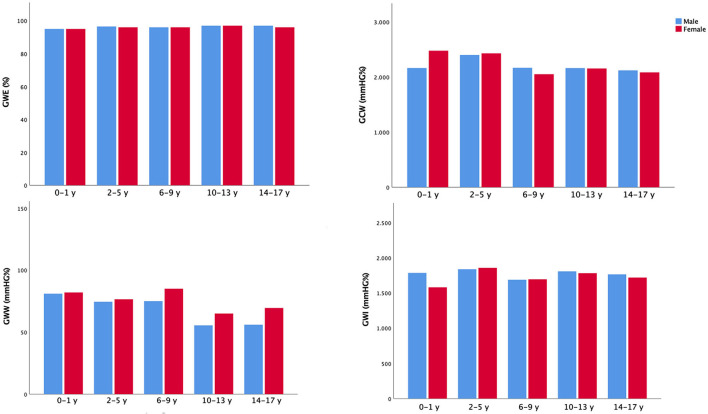
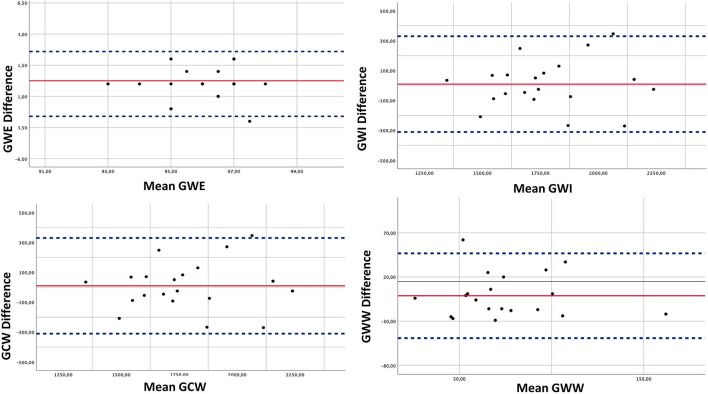
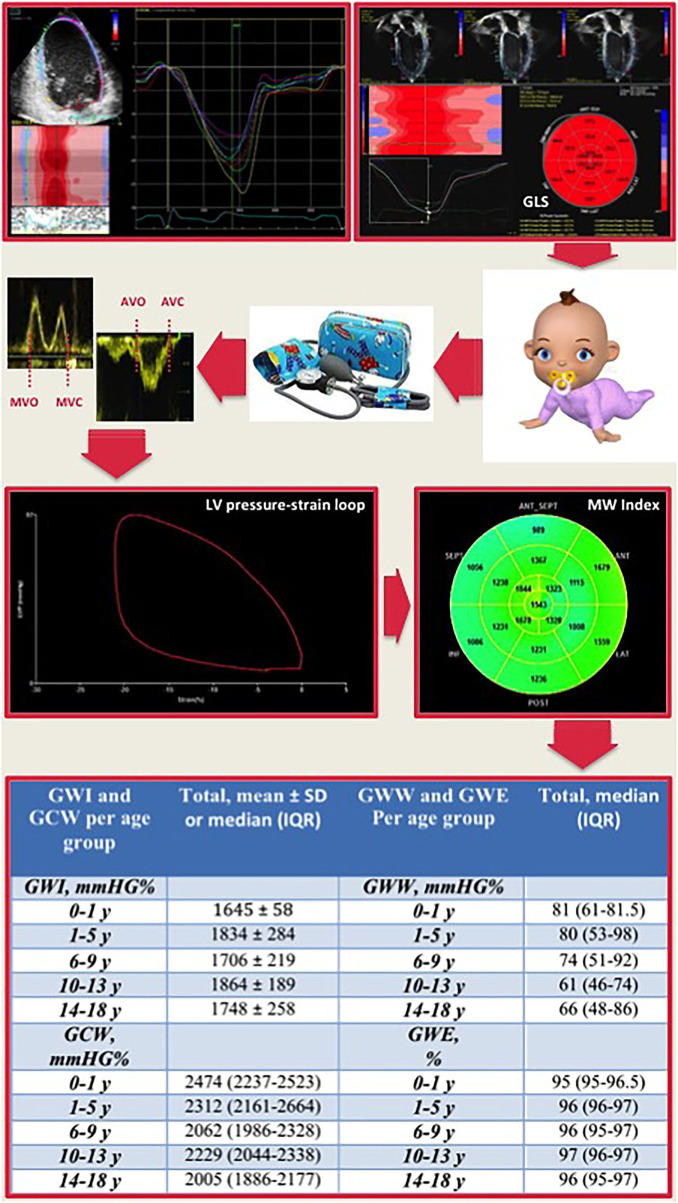
Methods and results: In this retrospective multi-center study involving three pediatric laboratories, 150 healthy children and adolescents (mean age of 10.6 ± 4.5, 91 males) were enrolled. A complete echocardiographic examination has been performed, including global longitudinal strain (GLS) assessment. The following parameters of non-invasive MW have been obtained through a dedicated software: global work index (GWI), global constructive work (GCW), global work waste (GWW), and global work efficiency (GWE), using left ventricular (LV) strain loops and non-invasive brachial artery cuff pressure values. The lowest expected values were for GWI 1,723 mmHg% in males and 1,682 mmHg% in females, for GCW 2,089 and 2,106 mmHg%, for GWE 95.9 and 95.5% whereas the highest expected value for GWW was 78 mmHg% in men and 90 mmHg% in women. The univariable and multivariable analysis showed significant associations between either GWI or GCW with SBP (β coefficient = 0.446, p < 0.001; β coefficient = 0.456, p < 0.001, respectively) and LV GLS (β coefficient = -0.268, p = 0.001; β coefficient = -0.233, p = 0.003, respectively). Inter- and intra-observer variability showed good reproducibility of non-invasive MW parameters.
Conclusion: Non-invasive MW parameters were feasible and reliable in the pediatric population. This study provided normal reference ranges of these useful echocardiographic indices.
Keywords: advanced echocardiography; congenital heart disease; myocardial work indices; speckle tracking analysis; systolic function.
Copyright © 2022 Sabatino, Leo, Strangio, Bella, Borrelli, Avesani, Josen, Paredes, Piccinelli, Sirico, Pergola, Fraisse, De Rosa, Indolfi and Di Salvo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Ersboll M, Valeur N, Mogensen UM, Andersen MJ, Moller JE, Velazquez EJ et al. Prediction of all-cause mortality and heart failure admissions from global left ventricular longitudinal strain in patients with acute myocardial infarction and preserved left ventricular ejection fraction. J Am Coll Cardiol. (2013) 61:2365–73. 10.1016/j.jacc.2013.02.061 - DOI - PubMed