

Socioeconomic Status and Prognosis of Patients With ST-Elevation Myocardial Infarction Managed by the Emergency-Intervention "Codi IAM" Network
- PMID: 35548422
- PMCID: PMC9082814
- DOI: 10.3389/fcvm.2022.847982
Socioeconomic Status and Prognosis of Patients With ST-Elevation Myocardial Infarction Managed by the Emergency-Intervention "Codi IAM" Network
Abstract
Background: Despite the spread of ST-elevation myocardial infarction (STEMI) emergency intervention networks, inequalities in healthcare access still have a negative impact on cardiovascular prognosis. The Family Income Ratio of Barcelona (FIRB) is a socioeconomic status (SES) indicator that is annually calculated. Our aim was to evaluate whether SES had an effect on mortality and complications in patients managed by the "Codi IAM" network in Barcelona.
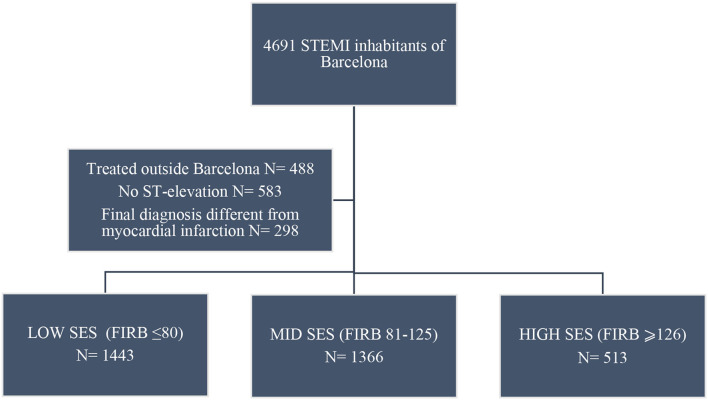
Methods: This is a cohort study with 3,322 consecutive patients with STEMI treated in Barcelona from 2010 to 2016. Collected data include treatment delays, clinical and risk factor characteristics, and SES. The patients were assigned to three SES groups according to FIRB score. A logistic regression analysis was conducted to estimate the adjusted effect of SES on 30-day mortality, 30-day composite cardiovascular end point, and 1-year mortality.
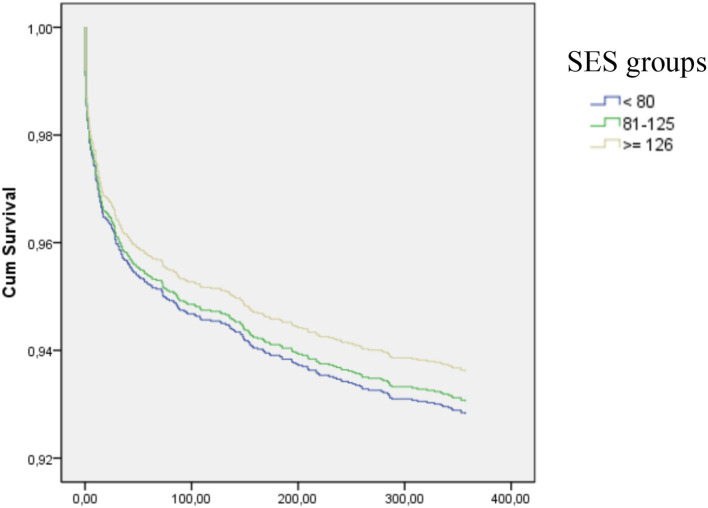
Results: The mean age of the patients was 65 ± 13% years, 25% were women, and 21% had diabetes mellitus. Patients with low SES were younger, more often hypertensive, diabetic, dyslipidemic (p < 0.003), had longer reperfusion delays (p < 0.03) compared to participants with higher SES. Low SES was not independently associated with 30-day mortality (OR: 0.95;9 5% CI: 0.7-1.3), 30-day cardiovascular composite end point (OR: 1.03; 95% CI: 0.84-1.26), or 1-year all-cause mortality (HR: 1.09; 95% CI: 0.76-1.56).
Conclusion: Although the low-SES patients with STEMI in Barcelona city were younger, had worse clinical profiles, and had longer revascularization delays, their 30-day and 1-year outcomes were comparable to those of the higher-SES patients.
Keywords: ST-elevation myocardial infarction; inequalities; mortality; primary percutaneous coronary intervention; reperfusion.
Copyright © 2022 Tizón-Marcos, Vaquerizo, Ferré, Farré, Lidón, Garcia-Picart, Regueiro, Ariza, Carrillo, Duran, Poirier, Cladellas, Camps-Vilaró, Ribas, Cubero-Gallego and Marrugat.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Differences in 30-day complications and 1-year mortality by sex in patients with a first STEMI managed by the Codi IAM network between 2010 and 2016.Rev Esp Cardiol (Engl Ed). 2021 Aug;74(8):674-681. doi: 10.1016/j.rec.2020.06.002. Epub 2020 Jul 11. Rev Esp Cardiol (Engl Ed). 2021. PMID: 32660910 English, Spanish.
-
Impact of Socioeconomic Status on Clinical Outcomes in Patients With ST-Segment-Elevation Myocardial Infarction.Circ Cardiovasc Qual Outcomes. 2019 Jan;12(1):e004979. doi: 10.1161/CIRCOUTCOMES.118.004979. Circ Cardiovasc Qual Outcomes. 2019. PMID: 30606051
-
Primary Ventricular Fibrillation in the Primary Percutaneous Coronary Intervention ST-Segment Elevation Myocardial Infarction Era (from the "Codi IAM" Multicenter Registry).Am J Cardiol. 2018 Aug 15;122(4):529-536. doi: 10.1016/j.amjcard.2018.04.054. Epub 2018 Jun 27. Am J Cardiol. 2018. PMID: 29960663
-
Sex Differences Persist in Time to Presentation, Revascularization, and Mortality in Myocardial Infarction Treated With Percutaneous Coronary Intervention.J Am Heart Assoc. 2019 May 21;8(10):e012161. doi: 10.1161/JAHA.119.012161. J Am Heart Assoc. 2019. PMID: 31092091 Free PMC article.
-
Prognostic value of access site and nonaccess site bleeding after percutaneous coronary intervention: a cohort study in ST-segment elevation myocardial infarction and comprehensive meta-analysis.JACC Cardiovasc Interv. 2014 Jun;7(6):622-30. doi: 10.1016/j.jcin.2014.01.162. Epub 2014 May 14. JACC Cardiovasc Interv. 2014. PMID: 24835321 Review.
Cited by
-
Socioeconomic Disparities and In-Hospital Outcomes in Acute Myocardial Infarction: A Case-Control Study.Cureus. 2025 May 6;17(5):e83551. doi: 10.7759/cureus.83551. eCollection 2025 May. Cureus. 2025. PMID: 40476103 Free PMC article.
References
-
- Organization WH . Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016. In: Organization WH , editor. Geneva: World Health Organization.
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. . 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39:119–77. 10.1093/eurheartj/ehx393 - DOI - PubMed