

Endoscopic bariatrics: current therapies and future directions
- PMID: 35548475
- PMCID: PMC9081914
- DOI: 10.21037/tgh.2020.03.09
Endoscopic bariatrics: current therapies and future directions
Abstract
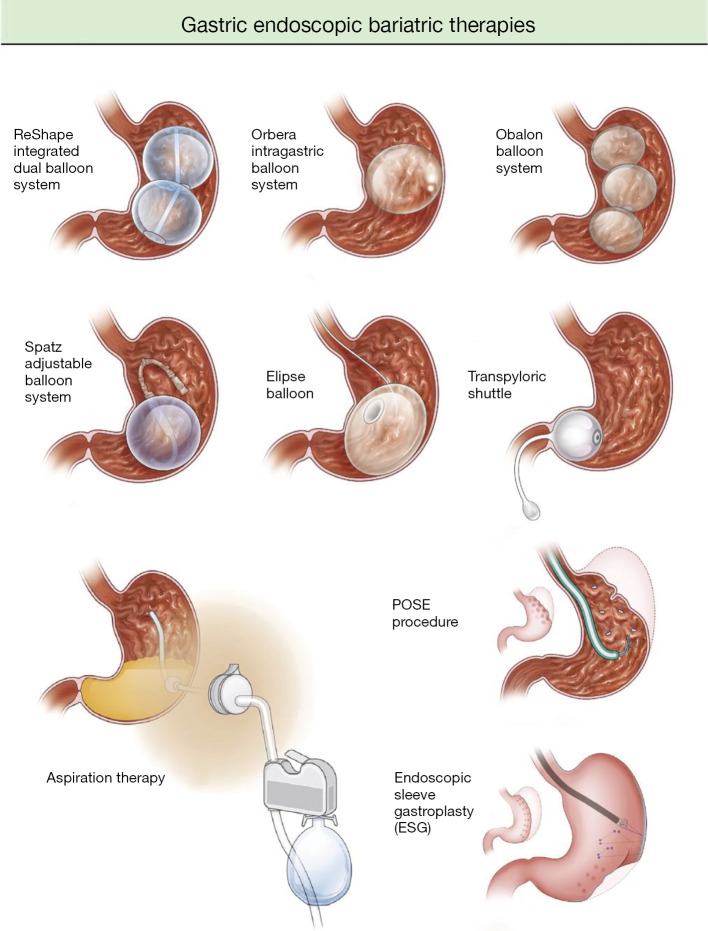
Endoscopic bariatric therapies (EBTs) are endoscopic procedures indicated for weight loss in the obese population. They are shown to be safe and effective for patients who do not quality for bariatric surgery. There are currently no randomized controlled studies comparing bariatric surgery with EBTs. However, EBTs are more cost effective and have fewer complications. This review will examine currently available EBTs with published data.
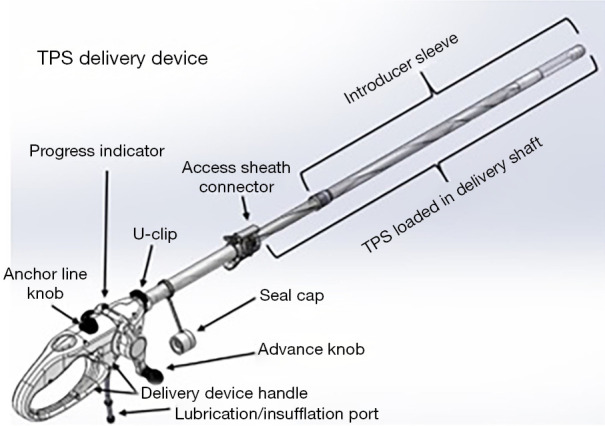
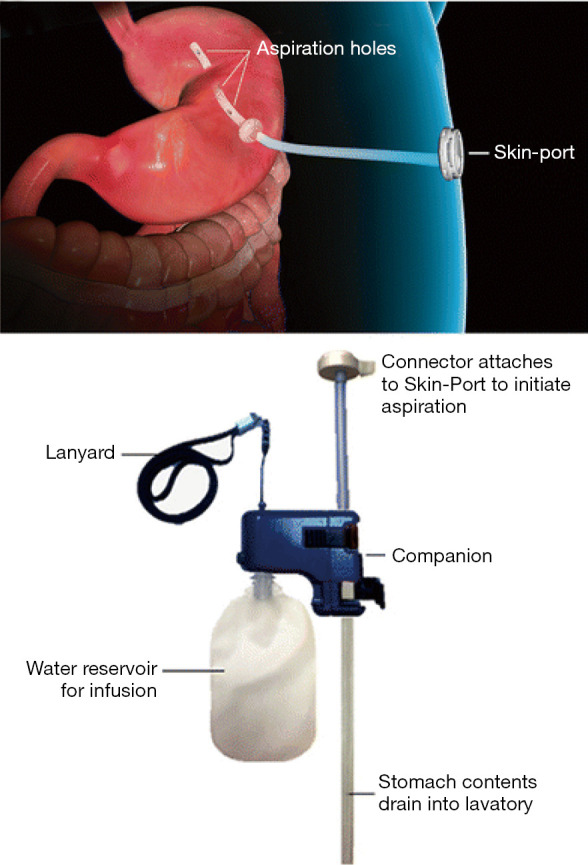
Keywords: Bariatric; aspiration; duodenal mucosal resurfacing; duodenal-jejunal bypass liner; endobariatric; endobarrier; endoscopic sleeve gastroplasty; endoscopy; gastro-duodeno-jejunal bypass sleeve; intragastric balloon (IGB); obesity; primary obesity surgery endoluminal (POSE); transoral outlet reduction (TORe); transpyloric shuttle (TPS).
2022 Translational Gastroenterology and Hepatology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tgh.amegroups.com/article/view/10.21037/tgh.2020.03.09/coif). The series “Innovation in Endoscopy” was commissioned by the editorial office without any funding or sponsorship. AS reports personal fees from Obalon, outside the submitted work. The authors have no other conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources