

Recall of preexisting cross-reactive B cell memory after Omicron BA.1 breakthrough infection
- PMID: 35549299
- PMCID: PMC9097882
- DOI: 10.1126/sciimmunol.abq3511
Recall of preexisting cross-reactive B cell memory after Omicron BA.1 breakthrough infection
Abstract
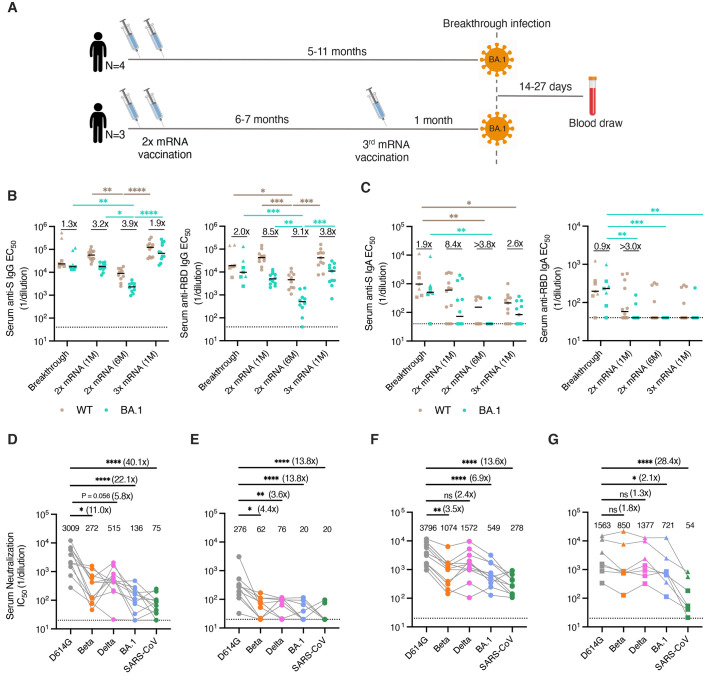
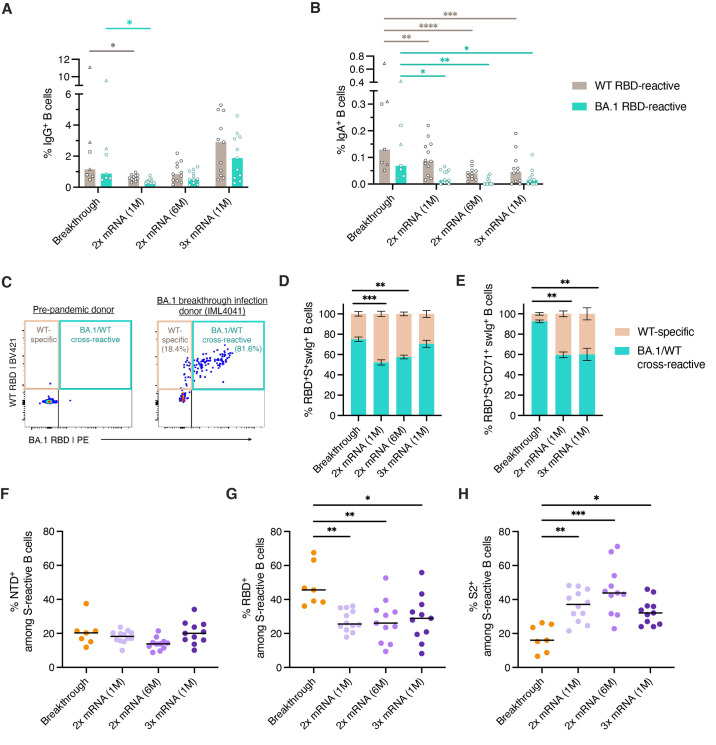
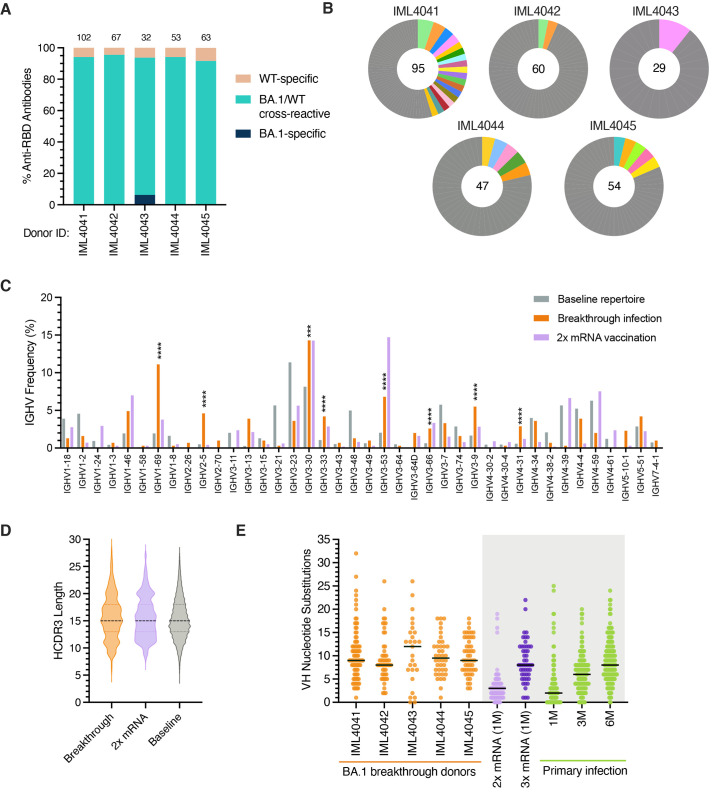
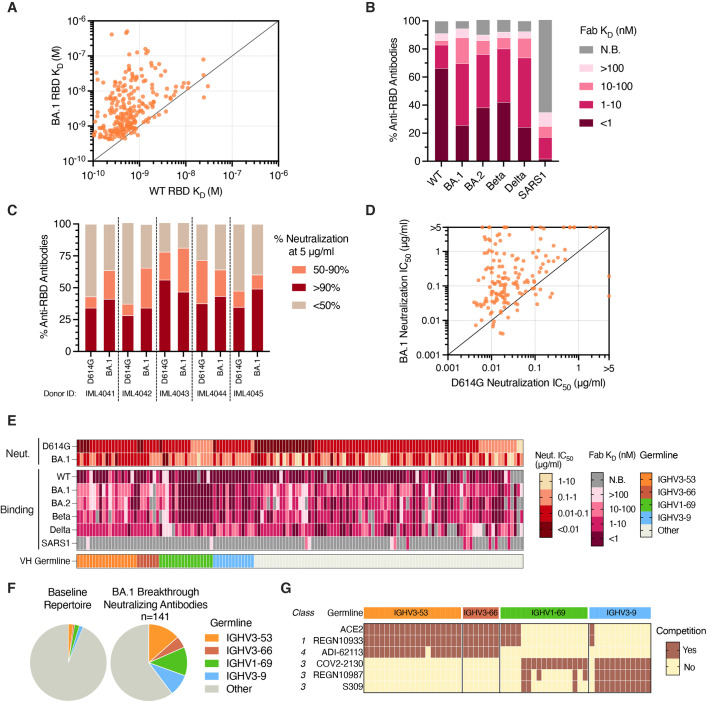
Understanding immune responses after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) breakthrough infection will facilitate the development of next-generation vaccines. Here, we profiled spike (S)-specific B cell responses after Omicron/BA.1 infection in messenger RNA-vaccinated donors. The acute antibody response was characterized by high levels of somatic hypermutation and a bias toward recognition of ancestral SARS-CoV-2 strains, suggesting the early activation of vaccine-induced memory B cells. BA.1 breakthrough infection induced a shift in B cell immunodominance hierarchy from the S2 subunit, which is highly conserved across SARS-CoV-2 variants of concern (VOCs), and toward the antigenically variable receptor binding domain (RBD). A large proportion of RBD-directed neutralizing antibodies isolated from BA.1 breakthrough infection donors displayed convergent sequence features and broadly recognized SARS-CoV-2 VOCs. Together, these findings provide insights into the role of preexisting immunity in shaping the B cell response to heterologous SARS-CoV-2 variant exposure.
Figures
Comment in
-
Immune memory to SARS-CoV-2 Omicron BA.1 breakthrough infections: To change the vaccine or not?Sci Immunol. 2022 Aug 26;7(74):eabq5901. doi: 10.1126/sciimmunol.abq5901. Epub 2022 Aug 26. Sci Immunol. 2022. PMID: 35653497
References
-
- Pilishvili T., Gierke R., Fleming-Dutra K. E., Farrar J. L., Mohr N. M., Talan D. A., Krishnadasan A., Harland K. K., Smithline H. A., Hou P. C., Lee L. C., Lim S. C., Moran G. J., Krebs E., Steele M. T., Beiser D. G., Faine B., Haran J. P., Nandi U., Schrading W. A., Chinnock B., Henning D. J., Lovecchio F., Lee J., Barter D., Brackney M., Fridkin S. K., Marceaux-Galli K., Lim S., Phipps E. C., Dumyati G., Pierce R., Markus T. M., Anderson D. J., Debes A. K., Lin M. Y., Mayer J., Kwon J. H., Safdar N., Fischer M., Singleton R., Chea N., Magill S. S., Verani J. R., Schrag S. J.; Vaccine Effectiveness among Healthcare Personnel Study Team , Effectiveness of mRNA Covid-19 Vaccine among U.S. Health Care Personnel. N. Engl. J. Med. 385, e90 (2021). 10.1056/NEJMoa2106599 - DOI - PMC - PubMed
-
- Feikin D. R., Higdon M. M., Abu-Raddad L. J., Andrews N., Araos R., Goldberg Y., Groome M. J., Huppert A., O’Brien K. L., Smith P. G., Wilder-Smith A., Zeger S., Deloria Knoll M., Patel M. K., Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 399, 924–944 (2022). 10.1016/S0140-6736(22)00152-0 - DOI - PMC - PubMed
-
- Pouwels K. B., Pritchard E., Matthews P. C., Stoesser N., Eyre D. W., Vihta K. D., House T., Hay J., Bell J. I., Newton J. N., Farrar J., Crook D., Cook D., Rourke E., Studley R., Peto T. E. A., Diamond I., Walker A. S., Effect of Delta variant on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. Nat. Med. 27, 2127–2135 (2021). 10.1038/s41591-021-01548-7 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
