

Development of the Revision Hip Complexity Classification using a modified Delphi technique
- PMID: 35549448
- PMCID: PMC9134833
- DOI: 10.1302/2633-1462.35.BJO-2022-0022.R1
Development of the Revision Hip Complexity Classification using a modified Delphi technique
Abstract
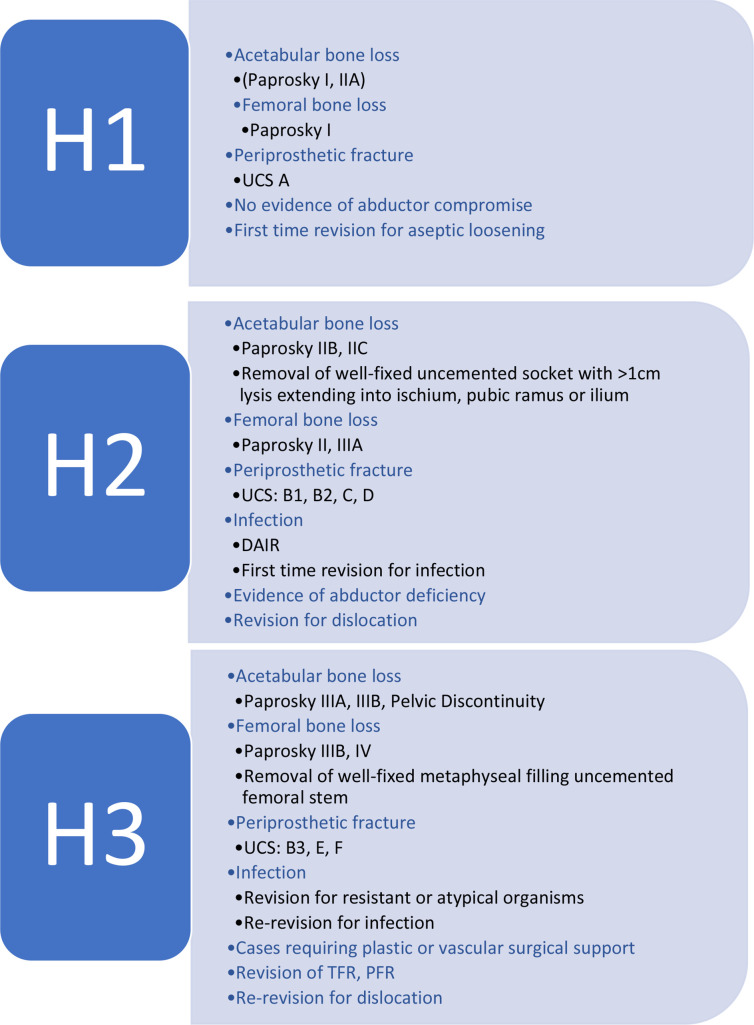
Aims: The aim of this modified Delphi process was to create a structured Revision Hip Complexity Classification (RHCC) which can be used as a tool to help direct multidisciplinary team (MDT) discussions of complex cases in local or regional revision networks.
Methods: The RHCC was developed with the help of a steering group and an invitation through the British Hip Society (BHS) to members to apply, forming an expert panel of 35. We ran a mixed-method modified Delphi process (three rounds of questionnaires and one virtual meeting). Round 1 consisted of identifying the factors that govern the decision-making and complexities, with weighting given to factors considered most important by experts. Participants were asked to identify classification systems where relevant. Rounds 2 and 3 focused on grouping each factor into H1, H2, or H3, creating a hierarchy of complexity. This was followed by a virtual meeting in an attempt to achieve consensus on the factors which had not achieved consensus in preceding rounds.
Results: The expert group achieved strong consensus in 32 out of 36 factors following the Delphi process. The RHCC used the existing Paprosky (acetabulum and femur), Unified Classification System, and American Society of Anesthesiologists (ASA) classification systems. Patients with ASA grade III/IV are recognized with a qualifier of an asterisk added to the final classification. The classification has good intraobserver and interobserver reliability with Kappa values of 0.88 to 0.92 and 0.77 to 0.85, respectively.
Conclusion: The RHCC has been developed through a modified Delphi technique. RHCC will provide a framework to allow discussion of complex cases as part of a local or regional hip revision MDT. We believe that adoption of the RHCC will provide a comprehensive and reproducible method to describe each patient's case with regard to surgical complexity, in addition to medical comorbidities that may influence their management. Cite this article: Bone Jt Open 2022;3(5):423-431.
Keywords: Anesthesiologists; Bone loss; Delphi methodology; Delphi process; Dislocation; Hip; Infection; Periprosthetic fracture; Revision Hip Complexity Classification; Revision total hip arthroplasty; acetabulum; bone loss; debridement, antibiotics, and implant retention; femur; medical comorbidities; periprosthetic fractures; revision hip surgery.
Figures


Similar articles
-
Financial analysis of revision hip surgery at a tertiary referral centre as classified using the British Hip Society Revision Hip Complexity Classification.Bone Jt Open. 2023 Aug 1;4(8):559-566. doi: 10.1302/2633-1462.48.BJO-2023-0004.R1. Bone Jt Open. 2023. PMID: 37524337 Free PMC article.
-
Modifiable risk factors for mortality in revision total hip arthroplasty for periprosthetic fracture.Bone Joint J. 2020 May;102-B(5):580-585. doi: 10.1302/0301-620X.102B5.BJJ-2019-1673.R1. Bone Joint J. 2020. PMID: 32349604
-
Impaction Bone Grafting for Severe Femoral Bone Loss: Surgical Technique in Revision Total Hip Arthroplasty.JBJS Essent Surg Tech. 2022 Feb 16;12(1):e20.00043. doi: 10.2106/JBJS.ST.20.00043. eCollection 2022 Jan-Mar. JBJS Essent Surg Tech. 2022. PMID: 35692723 Free PMC article.
-
Diagnosing Hip Microinstability: an international consensus study using the Delphi methodology.Knee Surg Sports Traumatol Arthrosc. 2023 Jan;31(1):40-49. doi: 10.1007/s00167-022-06933-4. Epub 2022 Apr 30. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 35499620 Free PMC article. Review.
-
Consensus minimum data set for lung cancer multidisciplinary teams: Results of a Delphi process.Respirology. 2018 Oct;23(10):927-934. doi: 10.1111/resp.13307. Epub 2018 Apr 11. Respirology. 2018. PMID: 29641841
Cited by
-
Financial analysis of revision hip surgery at a tertiary referral centre as classified using the British Hip Society Revision Hip Complexity Classification.Bone Jt Open. 2023 Aug 1;4(8):559-566. doi: 10.1302/2633-1462.48.BJO-2023-0004.R1. Bone Jt Open. 2023. PMID: 37524337 Free PMC article.
-
Periprosthetic hip infection: Current concepts and the Wrightington experience.J Clin Orthop Trauma. 2024 Jul 28;55:102509. doi: 10.1016/j.jcot.2024.102509. eCollection 2024 Aug. J Clin Orthop Trauma. 2024. PMID: 39184529 Free PMC article.
References
-
- Briggs T. A national review of adult elective orthopaedic services in England: GETTING IT RIGHT FIRST TIME. 2015. https://gettingitrightfirsttime.co.uk/wp-content/uploads/2018/07/GIRFT-N... (date last accessed 11 April 2022).
-
- Saklad M. Grading of patients for surgical procedures. Anesthesiol. 1941;5(2):281–284.
-
- Dalkey NC. Delphi. RAND Corporation. January 1967. https://www.rand.org/pubs/papers/P3704.html (date last accessed 29 March 2022).
LinkOut - more resources
Full Text Sources
Miscellaneous
