

Risks of Mortality and Airflow Limitation in Japanese Individuals with Preserved Ratio Impaired Spirometry
- PMID: 35549659
- PMCID: PMC9716906
- DOI: 10.1164/rccm.202110-2302OC
Risks of Mortality and Airflow Limitation in Japanese Individuals with Preserved Ratio Impaired Spirometry
Abstract
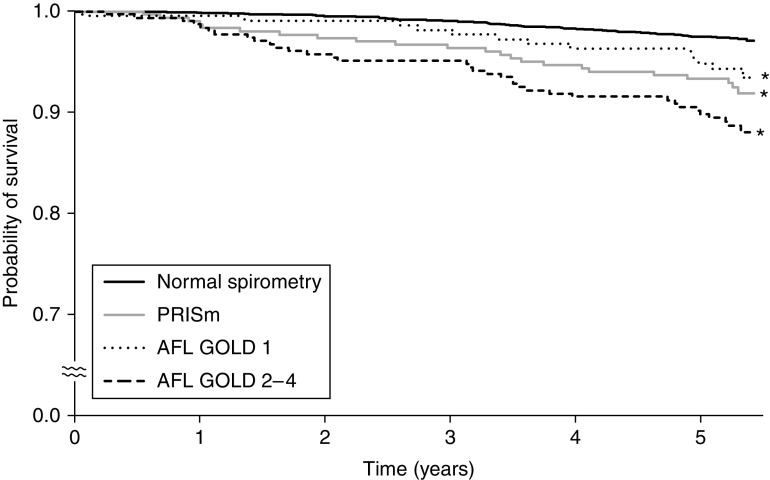
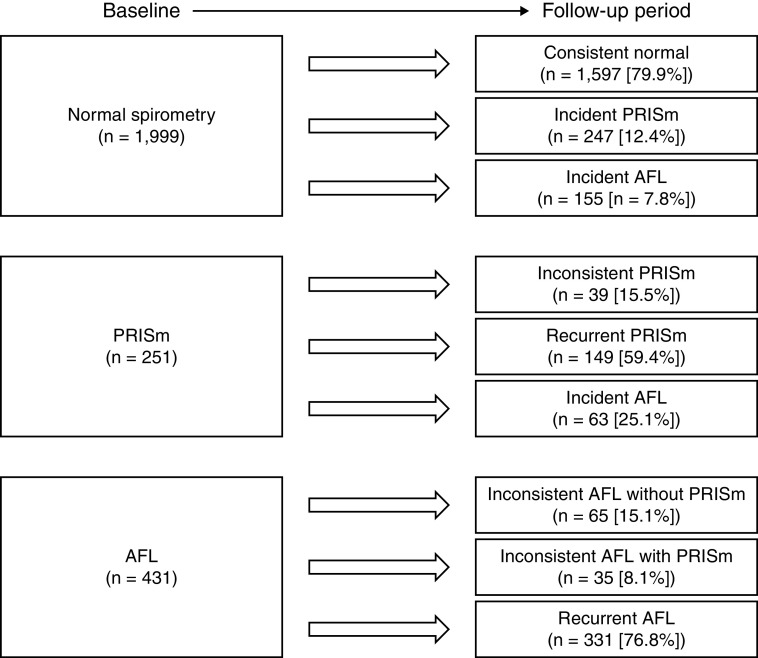
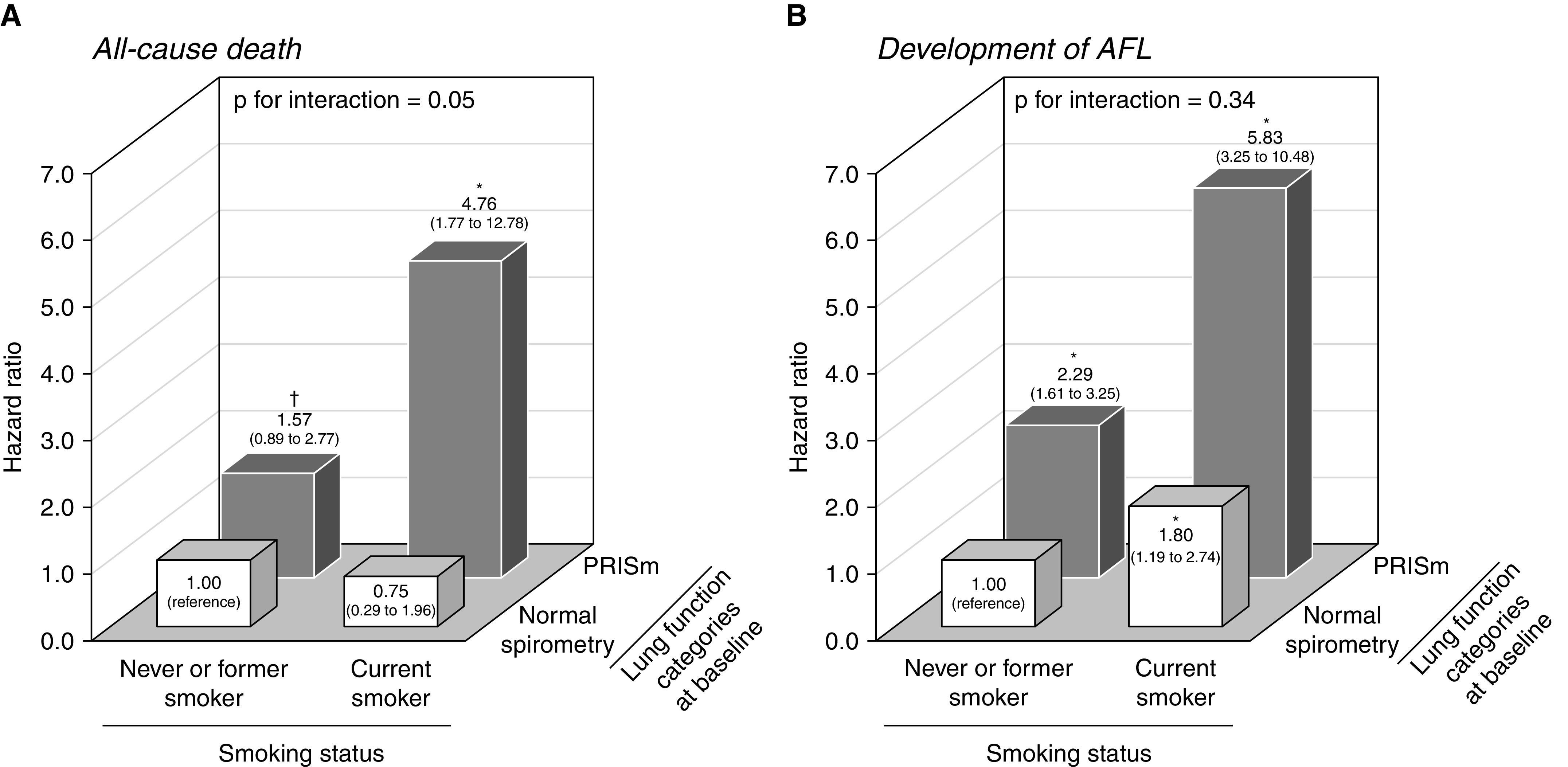
Rationale: Several Western studies have reported that participants with preserved ratio impaired spirometry (PRISm) have higher risks of airflow limitation (AFL) and death. However, evidence in East Asian populations is limited. Objectives: To investigate the relationship between PRISm and the risks of death and incident AFL in a Japanese population. Methods: A total of 3,032 community-dwelling Japanese participants aged ⩾40 years were seen in follow-up for a median of 5.3 years by annual spirometry examinations. Participants were classified into lung function categories at baseline as follows: normal spirometry (FEV1/FVC ⩾0.70 and FEV1 ⩾80% predicted), PRISm (⩾0.70 and <80%), AFL Global Initiative for Chronic Obstructive Lung Disease 1 (<0.70 and ⩾80%), and AFL Global Initiative for Chronic Obstructive Lung Disease 2-4 (<0.70 and <80%). Hazard ratios (HRs) and their 95% confidence intervals were computed using a Cox proportional hazards model. Measurements and Main Results: During the follow-up period, 131 participants died, 22 of whom died of cardiovascular disease, and 218 participants developed AFL. When examining the prognosis of each baseline lung function category, participants with PRISm had higher risks of all-cause death (HR, 2.20; 95% confidence interval, 1.35-3.59) and cardiovascular death (HR, 4.07; 1.07-15.42) than those with normal spirometry after adjusting for confounders. Moreover, the multivariable-adjusted risk of incident AFL was greater in participants with PRISm than in those with normal spirometry (HR, 2.48; 1.83-3.36). Conclusions: PRISm was associated with higher risks of all-cause and cardiovascular death and a greater risk of the development of AFL in a Japanese community.
Keywords: lung disease epidemiology; spirometry classification; spirometry mortality; spirometry statistics and numerical data.
Figures
Comment in
-
The Clinical Spectrum of PRISm.Am J Respir Crit Care Med. 2022 Sep 1;206(5):524-525. doi: 10.1164/rccm.202205-0965ED. Am J Respir Crit Care Med. 2022. PMID: 35612910 Free PMC article. No abstract available.
References
-
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med . 2017;5:691–706. - PMC - PubMed
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Am J Respir Crit Care Med . 2017;195:557–582. - PubMed
-
- Qaseem A, Wilt TJ, Weinberger SE, Hanania NA, Criner G, van der Molen T, et al. American College of Physicians; American College of Chest Physicians; American Thoracic Society; European Respiratory Society Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med . 2011;155:179–191. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
