

Outpatient Randomized Crossover Comparison of Zone Model Predictive Control Automated Insulin Delivery with Weekly Data Driven Adaptation Versus Sensor-Augmented Pump: Results from the International Diabetes Closed-Loop Trial 4
- PMID: 35549708
- PMCID: PMC9422791
- DOI: 10.1089/dia.2022.0084
Outpatient Randomized Crossover Comparison of Zone Model Predictive Control Automated Insulin Delivery with Weekly Data Driven Adaptation Versus Sensor-Augmented Pump: Results from the International Diabetes Closed-Loop Trial 4
Abstract
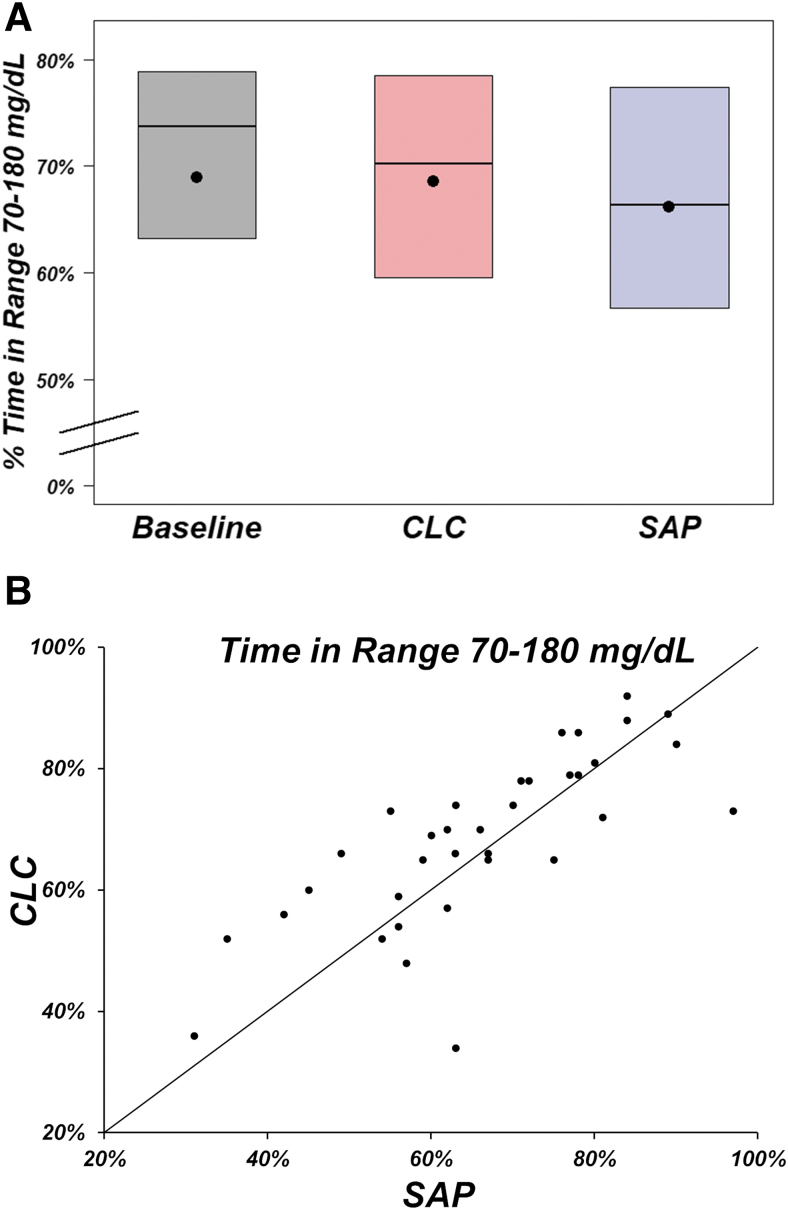
Background: Automated insulin delivery (AID) systems have proven effective in increasing time-in-range during both clinical trials and real-world use. Further improvements in outcomes for single-hormone (insulin only) AID may be limited by suboptimal insulin delivery settings. Methods: Adults (≥18 years of age) with type 1 diabetes were randomized to either sensor-augmented pump (SAP) (inclusive of predictive low-glucose suspend) or adaptive zone model predictive control AID for 13 weeks, then crossed over to the other arm. Each week, the AID insulin delivery settings were sequentially and automatically updated by an adaptation system running on the study phone. Primary outcome was sensor glucose time-in-range 70-180 mg/dL, with noninferiority in percent time below 54 mg/dL as a hierarchical outcome. Results: Thirty-five participants completed the trial (mean age 39 ± 16 years, HbA1c at enrollment 6.9% ± 1.0%). Mean time-in-range 70-180 mg/dL was 66% with SAP versus 69% with AID (mean adjusted difference +2% [95% confidence interval: -1% to +6%], P = 0.22). Median time <70 mg/dL improved from 3.0% with SAP to 1.6% with AID (-1.5% [-2.4% to -0.5%], P = 0.002). The adaptation system decreased initial basal rates by a median of 4% (-8%, 16%) and increased initial carbohydrate ratios by a median of 45% (32%, 59%) after 13 weeks. Conclusions: Automated adaptation of insulin delivery settings with AID use did not significantly improve time-in-range in this very well-controlled population. Additional study and further refinement of the adaptation system are needed, especially in populations with differing degrees of baseline glycemic control, who may show larger benefits from adaptation.
Keywords: Adaptation; Artificial pancreas; Automated insulin delivery; Glycemic control; Type 1 diabetes.
Conflict of interest statement
J.E.P. is currently an employee and shareholder of Tandem Diabetes Care, Inc., and has a significant financial interest in Tandem Diabetes Care. The work presented in the article was performed as part of his academic appointment at Sansum Diabetes Research Institute and is independent of his employment with Tandem Diabetes Care. E.D. reports receiving grants from JDRF, NIH, and Helmsley Charitable Trust, personal fees from Roche and Eli Lilly, patents on artificial pancreas technology, pending US Patent 62/686,931 and product support from Dexcom, Insulet, Tandem, and Roche. E.D. is currently an employee and shareholder of Eli Lilly and Company. The work presented in this manuscript was performed as part of his academic appointment and is independent of his employment with Eli Lilly and Company. C.J.L. reports grants paid to her institution from the National Institutes of Health, Insulet, Dexcom, Abbott, the Juvenile Diabetes Research Foundation, and AECOM; receiving consultancy fees from Dexcom and Eli Lilly; and serving on the Data Safety Monitoring Board (DSMB) for the Juvenile Diabetes Research Foundation and National Institutes of Health.
H.D. reports receiving consultancy fees from Guidepoint Consulting. L.E. reports receiving consultancy fees from Tandem Diabetes Care and Ypsomed. F.J.D. reports receiving royalties or license fees from ModeAGC, Roche, Dexcom, and Insult, advisory board for ModeAGC, and pending US Patent 62/686,931. All other authors report no conflict of interest related to this article.
Figures
References
-
- Bergenstal RM, Garg S, Weinzimer SA, et al. : Safety of a hybrid closed-loop insulin delivery system in patients with type 1 diabetes. JAMA 2016;316:1407–1408. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
