

Patient disposition using the Emergency Severity Index: a retrospective observational study at an interdisciplinary emergency department
- PMID: 35551090
- PMCID: PMC9109098
- DOI: 10.1136/bmjopen-2021-057684
Patient disposition using the Emergency Severity Index: a retrospective observational study at an interdisciplinary emergency department
Abstract
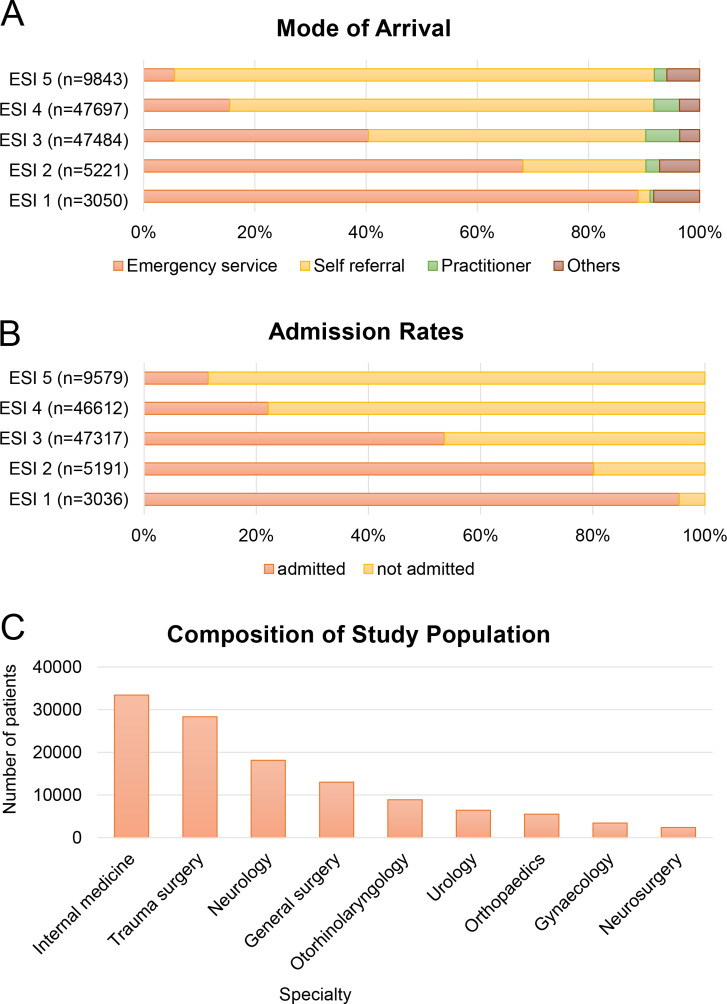
Objectives: Early patient disposition is crucial to prevent crowding in emergency departments (EDs). Our study aimed to characterise the need of in-house resources for patients treated in the ED according to the Emergency Severity Index (ESI) and the presenting complaint at the timepoint of triage.
Design: A retrospective single-centre study was conducted.
Setting: Data of all patients who presented to the interdisciplinary ED of a tertiary care hospital in Munich, Germany, from 2014 to 2017 were analysed.
Participants: n=113 694 patients were included.
Measures: ESI Score, medical speciality according to the chief complaint, mode of arrival, admission rates and discharge destination from the ED were evaluated.
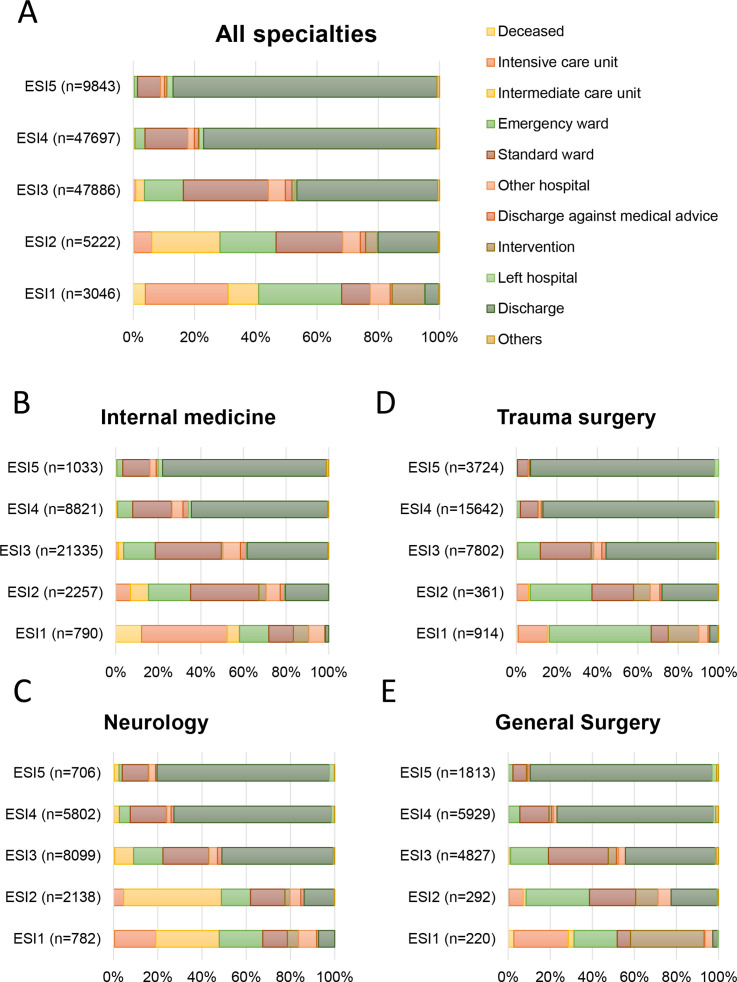
Results: Patient disposition varied according to ESI scores in combination with the chief complaint. Patients with low ESI scores were more likely to be admitted after treatment in the ED than patients with high ESI scores. Highly prioritised patients (ESI 1) mainly required admission to an intensive care unit (ICU, 27%), intermediate care unit (IMC, 37%) or immediate intervention (11%). In this critical patient group, 30% of patients with neurological or medical symptoms required immediate intensive care, whereas only 17% of patients with surgical problems were admitted to an ICU. A significant number of patients (particularly with neurological or medical problems) required hospital (and in some cases even ICU or IMC) admission despite high ESI scores.
Conclusions: Overall, ESI seems to be a useful tool to anticipate the need for specialised in-hospital resources on arrival. Patients with symptoms pointing at neurological or medical problems need particular attention as ESI may fail to sufficiently predict the care facility level for this patient group.
Keywords: accident & emergency medicine; adult intensive & critical care.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Mackway-Jones K. Emergency triage: Manchester triage group. BMJ Publishing Group, 1997.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources