

Safety and Efficacy of the mTOR Inhibitor, Vistusertib, Combined With Anastrozole in Patients With Hormone Receptor-Positive Recurrent or Metastatic Endometrial Cancer: The VICTORIA Multicenter, Open-label, Phase 1/2 Randomized Clinical Trial
- PMID: 35551299
- PMCID: PMC9100474
- DOI: 10.1001/jamaoncol.2022.1047
Safety and Efficacy of the mTOR Inhibitor, Vistusertib, Combined With Anastrozole in Patients With Hormone Receptor-Positive Recurrent or Metastatic Endometrial Cancer: The VICTORIA Multicenter, Open-label, Phase 1/2 Randomized Clinical Trial
Abstract
Importance: Endometrial cancer is often hormone-dependent and treated with aromatase inhibitors. The PI3K-AKT-mTOR pathway deregulation observed in endometrial cancer drives hormonal resistance, thus supporting the rationale of combining mTOR inhibitor with endocrine therapy.
Objective: To evaluate the safety and efficacy of vistusertib in combination with anastrozole in the treatment of women with hormone receptor-positive recurrent or metastatic endometrial cancer.
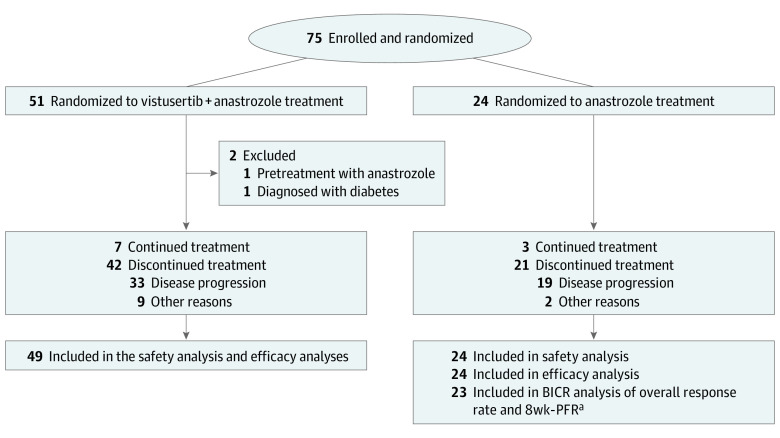
Design, settings, and participants: The VICTORIA study was a multicenter, open-label, randomized clinical trial that accrued 75 patients with hormone receptor-positive recurrent or metastatic endometrial cancer from 12 cancer centers in France in April 2016 to October 2019. After a safety run-in period, a Simon 2-stage design was used. Data analyses were performed from December 11, 2020, to March 11, 2021.
Interventions: Patients were randomized in a 2:1 ratio to oral vistusertib (125 mg twice daily 2 days per week) and oral anastrozole (1 mg daily) in the combination vistusertib with anastrozole arm (V+A arm) or oral anastrozole alone (A arm).
Main outcomes and measures: The primary end point was serious adverse events for the safety run-in period and progression-free rate at 8 weeks (8wk-PFR)-assessed with a blinded independent central review in phase 2. The secondary end points were objective response rate, duration of response, progression-free survival (PFS), overall survival, and incidence of adverse events.
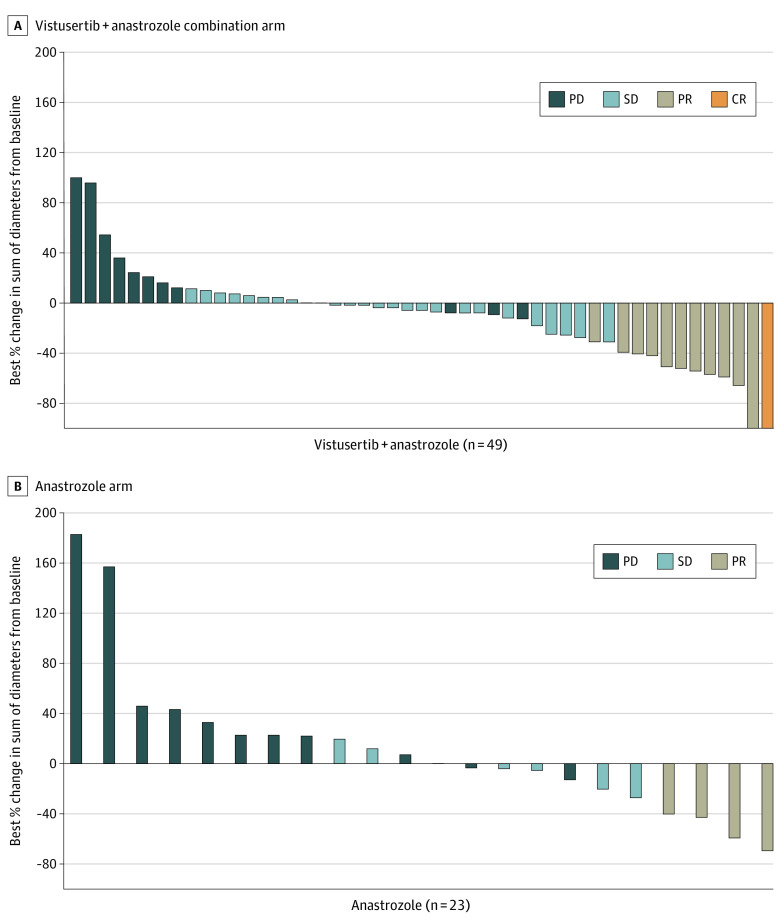
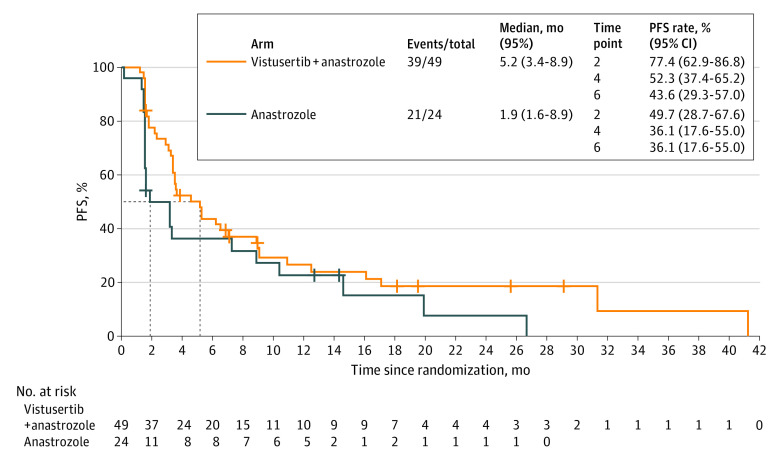
Results: Of the 75 patients who were randomized, 73 (median [range] age, 69.5 [37-88] y; all female) were treated: V+A arm, 49 patients; A arm, 24 patients. In the V+A arm, the 8wk-PFR was 67.3% (unilateral 95% CI, 54.7%) and in the A arm, 39.1% (unilateral 95% CI, 22.2%). No significant serious adverse events were reported during the safety run-in period (n = 6 in V+A arm). The overall response rate was 24.5% (95% CI, 13.3%-38.9%) in the V+A arm vs 17.4% (95% CI, 5.0%-38.8%) in the A arm. With a median follow-up of 27.7 months, median PFS was 5.2 (95% CI, 3.4-8.9) in the V+A arm and 1.9 (95% CI, 1.6-8.9) months in the A arm. Fatigue, lymphopenia, hyperglycemia, and diarrhea were the most common (grade ≥2) adverse events associated with vistusertib.
Conclusions and relevance: This multicenter, open-label, phase 1/2 randomized clinical trial demonstrated that adding vistusertib to anastrozole improved 8wk-PFR, overall response rate, and PFS for patients with endometrial cancer and had manageable adverse events. Identification of molecular subgroups would allow for more precise selection of patients who may be most likely to experience favorable outcomes.
Trial registration: ClinicalTrials.gov Identifier: NCT02730923.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
