

Association Between Visual Acuity and Residual Retinal Fluid Following Intravitreal Anti-Vascular Endothelial Growth Factor Treatment for Neovascular Age-Related Macular Degeneration: A Systematic Review and Meta-analysis
- PMID: 35551359
- PMCID: PMC9100487
- DOI: 10.1001/jamaophthalmol.2022.1357
Association Between Visual Acuity and Residual Retinal Fluid Following Intravitreal Anti-Vascular Endothelial Growth Factor Treatment for Neovascular Age-Related Macular Degeneration: A Systematic Review and Meta-analysis
Abstract
Importance: The association between residual subretinal fluid (SRF) and intraretinal fluid (IRF) and visual acuity following anti-vascular endothelial growth factor (VEGF) treatment is not well understood.
Objective: To examine the association of residual retinal fluid, SRF, and IRF with visual acuity following anti-VEGF treatment in patients with neovascular age-related macular degeneration (nAMD).
Data sources: A systematic literature search was performed from January 2005 to August 2021 using Ovid MEDLINE, Embase, and the Cochrane Library.
Study selection: Peer-reviewed articles reporting on visual acuity stratified by the presence or absence of any residual SRF, IRF, or any retinal fluid at last study observation after intravitreal bevacizumab, ranibizumab, aflibercept, or brolucizumab in patients with nAMD were included. Studies that were noncomparative, included fewer than 10 eyes, or reported on other anti-VEGF agents were excluded.
Data extraction and synthesis: Two independent reviewers conducted data extraction and synthesis. The Cochrane risk of bias tool 2 and ROBINS-I were used to assess risk of bias and GRADE evaluation was conducted to assess certainty of evidence.
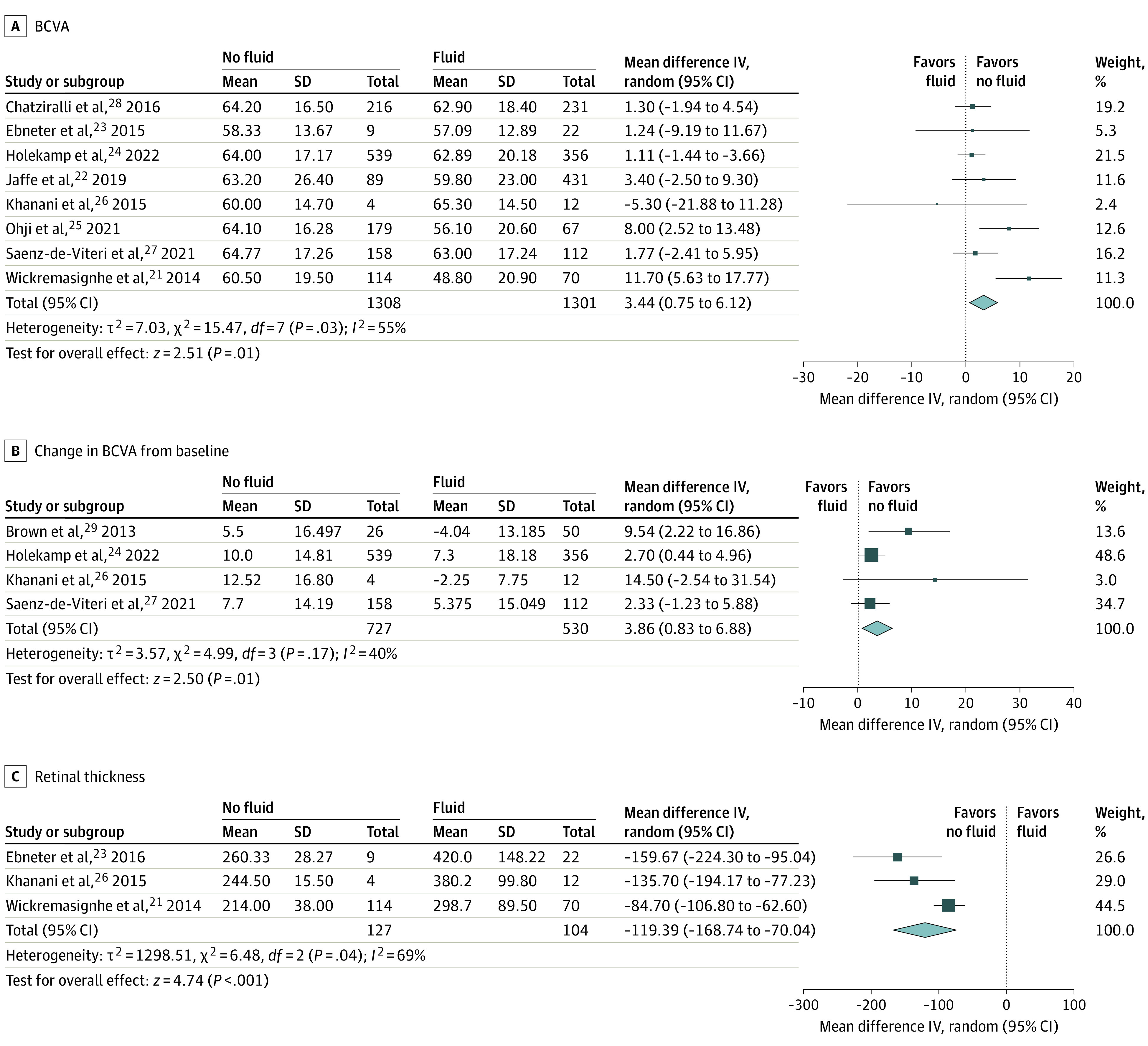
Main outcomes and measures: Primary outcomes were BCVA at last study observation, change in BCVA from baseline, and retinal thickness at last study observation.
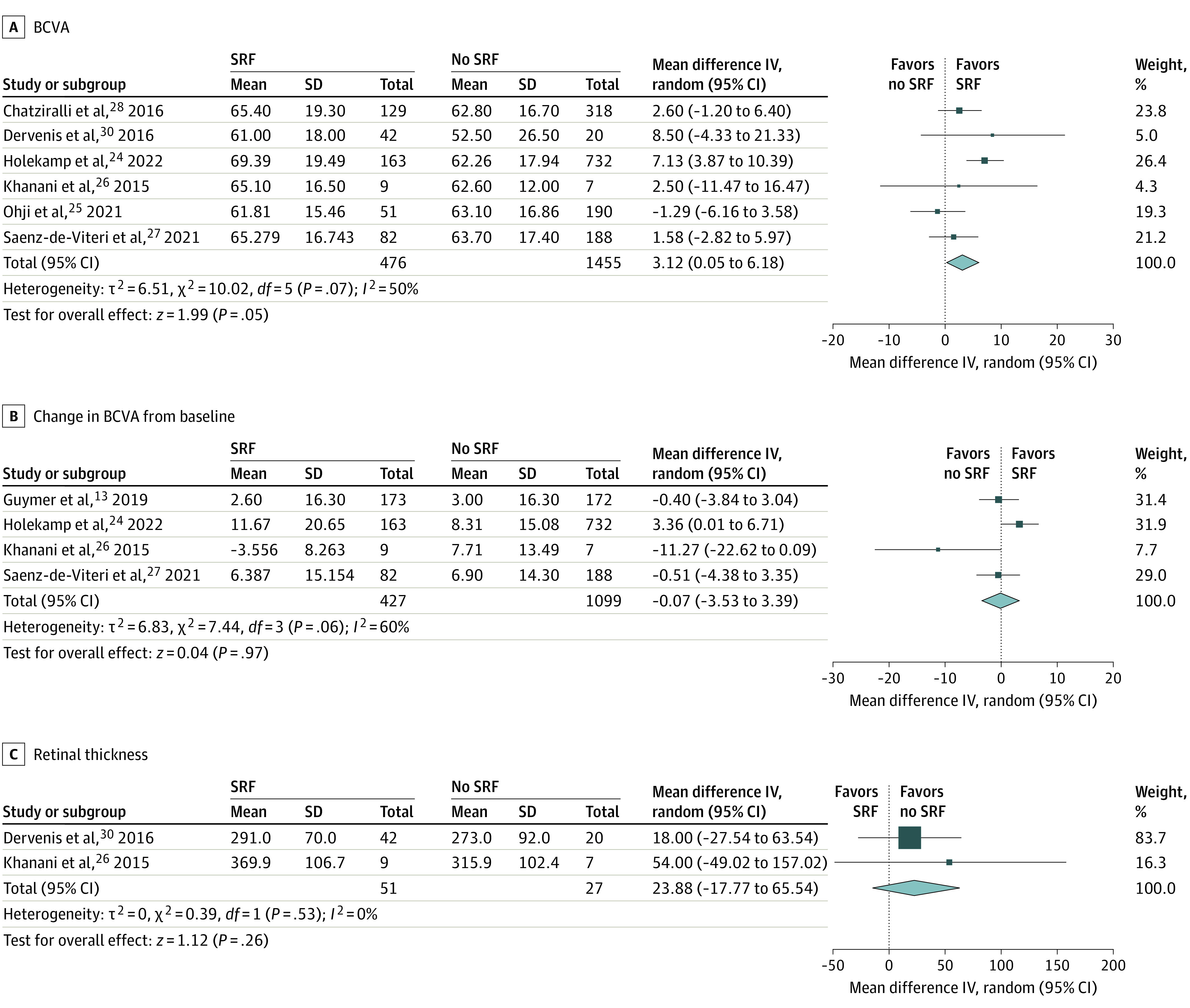
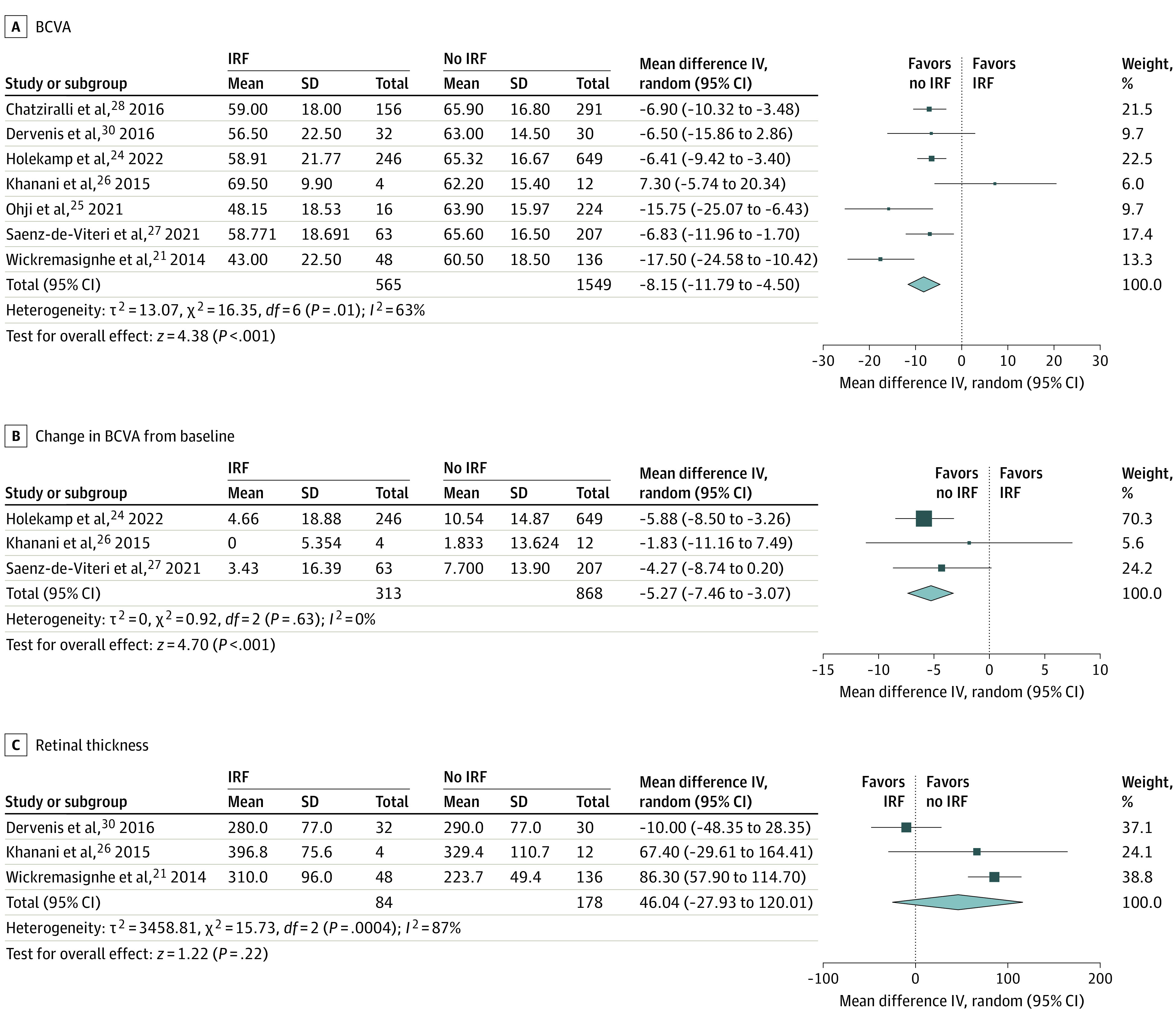
Results: In this systematic review and meta-analysis, 11 studies (6 randomized clinical trials [RCTs]) comprising 3092 eyes were included in our analysis. Across all included studies, the BCVA of eyes with residual SRF was better than eyes without SRF (weighted mean difference [WMD], 3.1 letter score; 95% CI, 0.05 to 6.18; P = .05; GRADE, low certainty of evidence; 6 studies; 1931 eyes) but similar in RCTs (WMD, 2.7 letter score; 95% CI, -2.40 to 7.84; P = .30; GRADE, low certainty of evidence; 3 studies; 1406 eyes). The BCVA of eyes with residual IRF was worse than that of eyes without IRF (WMD, -8.2 letter score; 95% CI, -11.79 to -4.50; P < .001; GRADE, low; 7 studies; 2114 eyes).
Conclusions and relevance: The findings suggest that the presence of residual SRF was associated with slightly better BCVA at last study observation; however, baseline differences in BCVA existed and this conclusion was primarily driven by 1 study. The presence of residual IRF was associated with substantially worse BCVA at last study observation and less improvement of BCVA from baseline. The conclusions are limited by the inclusion of data from observational studies, heterogeneity, and a low certainty of evidence.
Conflict of interest statement
Figures
Similar articles
-
Persistence of Retinal Fluid after Anti-VEGF Treatment for Neovascular Age-Related Macular Degeneration: A Systematic Review and Meta-Analysis.Ophthalmol Retina. 2025 Jul;9(7):603-617. doi: 10.1016/j.oret.2025.01.010. Epub 2025 Jan 20. Ophthalmol Retina. 2025. PMID: 39842717
-
Effect of Residual Retinal Fluid on Visual Function in Ranibizumab-Treated Neovascular Age-Related Macular Degeneration.Am J Ophthalmol. 2022 Jan;233:8-17. doi: 10.1016/j.ajo.2021.06.029. Epub 2021 Jul 18. Am J Ophthalmol. 2022. PMID: 34289338 Clinical Trial.
-
Retinal Fluid and Thickness Fluctuations in Archway Trial for Port Delivery System with Ranibizumab versus Monthly Ranibizumab Injections.Ophthalmol Retina. 2025 Apr;9(4):330-342. doi: 10.1016/j.oret.2024.10.015. Epub 2024 Oct 22. Ophthalmol Retina. 2025. PMID: 39447871 Clinical Trial.
-
Relationship between retinal fluid characteristics and vision in neovascular age-related macular degeneration: HARBOR post hoc analysis.Graefes Arch Clin Exp Ophthalmol. 2022 Dec;260(12):3781-3789. doi: 10.1007/s00417-022-05716-4. Epub 2022 Jun 10. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 35687173 Free PMC article. Clinical Trial.
-
Treatment regimens for administration of anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration.Cochrane Database Syst Rev. 2020 May 5;5(5):CD012208. doi: 10.1002/14651858.CD012208.pub2. Cochrane Database Syst Rev. 2020. PMID: 32374423 Free PMC article.
Cited by
-
Impact of Routinely Performed Optical Coherence Tomography Examinations on Quality of Life in Patients with Retinal Diseases-Results from the ALBATROS Data Collection.J Clin Med. 2023 Jun 7;12(12):3881. doi: 10.3390/jcm12123881. J Clin Med. 2023. PMID: 37373576 Free PMC article.
-
Treating or tolerating persistent subretinal fluid in neovascular age-related macular degeneration: a systematic review of visual and anatomical outcomes with anti-VEGF therapy.Int Ophthalmol. 2025 Apr 12;45(1):154. doi: 10.1007/s10792-025-03503-8. Int Ophthalmol. 2025. PMID: 40220174
-
To Treat or Not to Treat? Resolving the Question of Subretinal and Intraretinal Fluid in Age-Related Macular Degeneration: A Narrative Review.Ophthalmol Ther. 2025 Mar;14(3):489-514. doi: 10.1007/s40123-025-01093-3. Epub 2025 Feb 4. Ophthalmol Ther. 2025. PMID: 39904844 Free PMC article. Review.
-
Deep-Learning-Assisted Analysis of Early Biomarker Changes in Treatment-Naïve Patients with Neovascular AMD Under Intravitreal Faricimab.Ophthalmol Ther. 2025 May;14(5):1025-1037. doi: 10.1007/s40123-025-01125-y. Epub 2025 Mar 25. Ophthalmol Ther. 2025. PMID: 40133689 Free PMC article.
-
Practice patterns and preferences in the management of age-related macular degeneration among vitreoretinal surgeons in the Philippines.Int Ophthalmol. 2025 Feb 11;45(1):71. doi: 10.1007/s10792-025-03441-5. Int Ophthalmol. 2025. PMID: 39934587
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
