

Central sleep apnea: pathophysiologic classification
- PMID: 35551411
- PMCID: PMC9995798
- DOI: 10.1093/sleep/zsac113
Central sleep apnea: pathophysiologic classification
Abstract
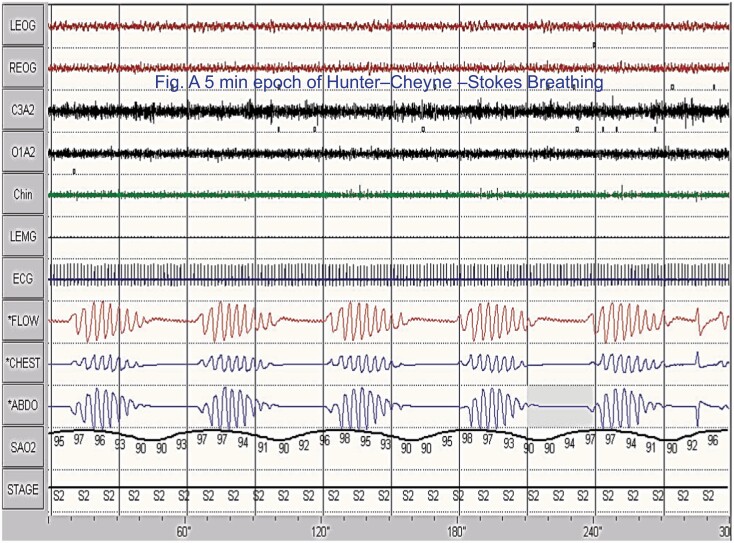
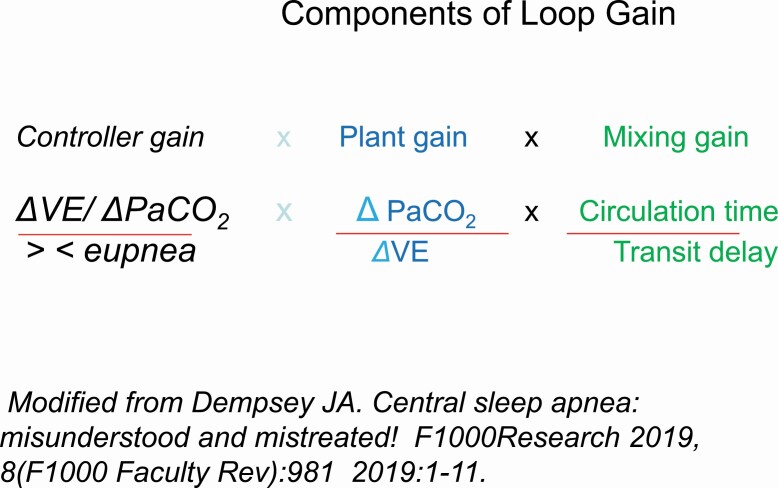
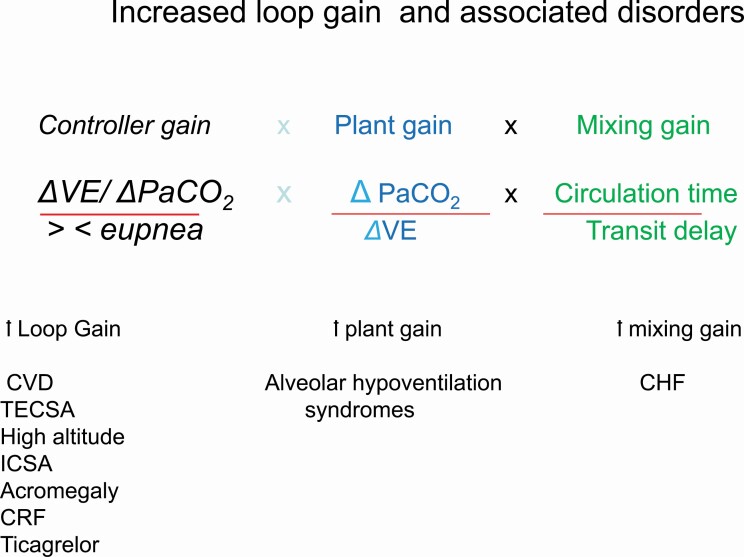
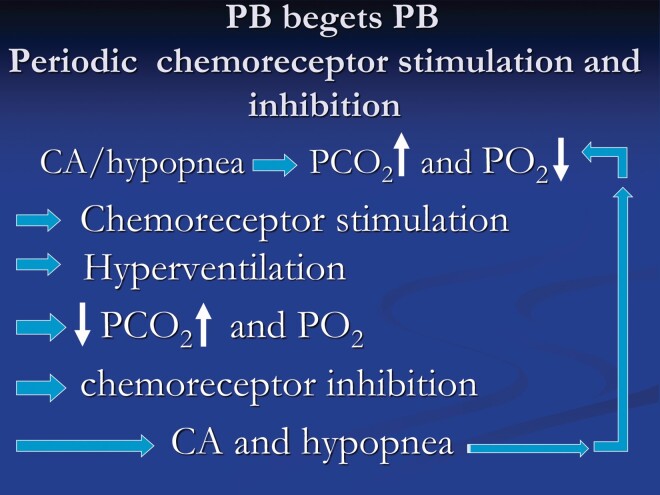
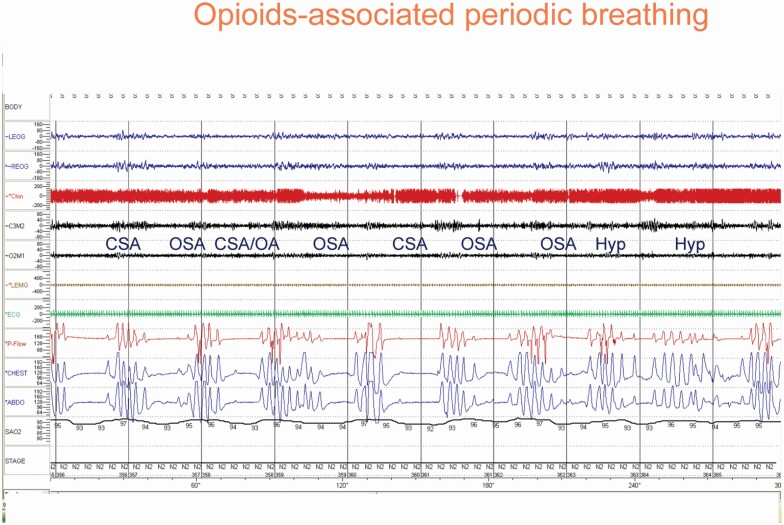
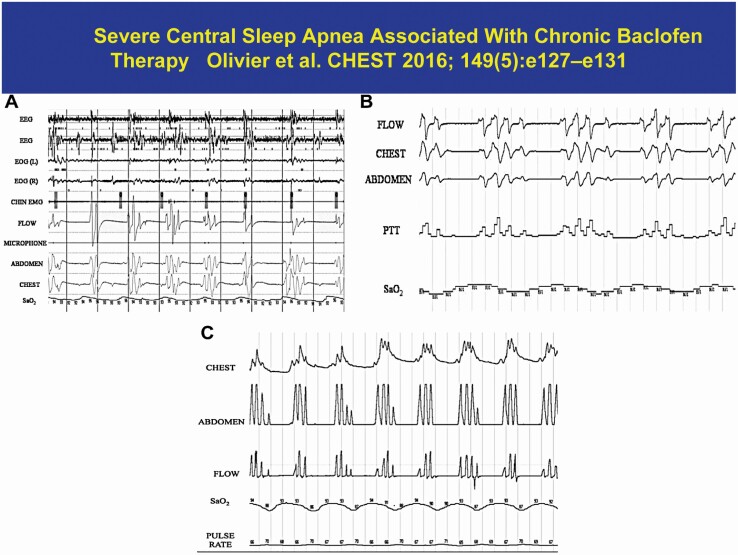
Central sleep apnea is not a single disorder; it can present as an isolated disorder or as a part of other clinical syndromes. In some conditions, such as heart failure, central apneic events are due to transient inhibition of ventilatory motor output during sleep, owing to the overlapping influences of sleep and hypocapnia. Specifically, the sleep state is associated with removal of wakefulness drive to breathe; thus, rendering ventilatory motor output dependent on the metabolic ventilatory control system, principally PaCO2. Accordingly, central apnea occurs when PaCO2 is reduced below the "apneic threshold". Our understanding of the pathophysiology of central sleep apnea has evolved appreciably over the past decade; accordingly, in disorders such as heart failure, central apnea is viewed as a form of breathing instability, manifesting as recurrent cycles of apnea/hypopnea, alternating with hyperpnea. In other words, ventilatory control operates as a negative-feedback closed-loop system to maintain homeostasis of blood gas tensions within a relatively narrow physiologic range, principally PaCO2. Therefore, many authors have adopted the engineering concept of "loop gain" (LG) as a measure of ventilatory instability and susceptibility to central apnea. Increased LG promotes breathing instabilities in a number of medical disorders. In some other conditions, such as with use of opioids, central apnea occurs due to inhibition of rhythm generation within the brainstem. This review will address the pathogenesis, pathophysiologic classification, and the multitude of clinical conditions that are associated with central apnea, and highlight areas of uncertainty.
Keywords: Adaptive-Servo Ventilation (ASV); apneic threshold; bi-level positive pressure therapy (BPAP); central apnea; continuous positive pressure therapy (CPAP); controller gain; hypocapnia; loop gain; plant gain.
© The Author(s) 2022. Published by Oxford University Press on behalf of Sleep Research Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
