

Propensity score-matched analysis comparing dose-escalated intensity-modulated radiation therapy versus external beam radiation therapy plus high-dose-rate brachytherapy for localized prostate cancer
- PMID: 35551434
- PMCID: PMC9300494
- DOI: 10.1007/s00066-022-01953-y
Propensity score-matched analysis comparing dose-escalated intensity-modulated radiation therapy versus external beam radiation therapy plus high-dose-rate brachytherapy for localized prostate cancer
Abstract
Purpose: Dose-escalated external beam radiation therapy (EBRT) and EBRT + high-dose-rate brachytherapy (HDR-BT) boost are guideline-recommended treatment options for localized prostate cancer. The purpose of this study was to compare long-term outcome and toxicity of dose-escalated EBRT versus EBRT + HDR-BT boost.
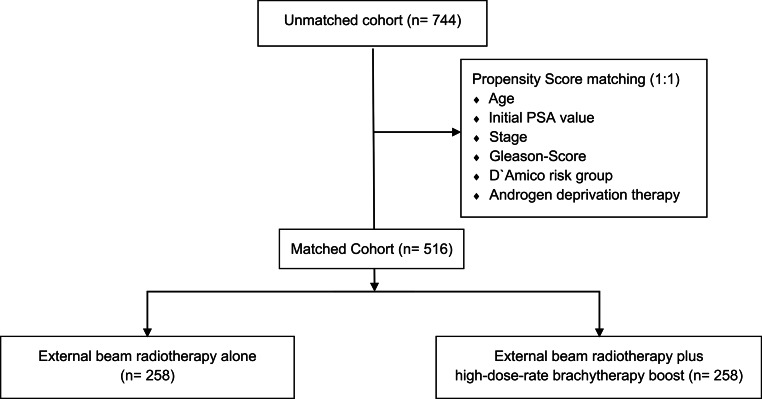
Methods: From 2002 to 2019, 744 consecutive patients received either EBRT or EBRT + HDR-BT boost, of whom 516 patients were propensity score matched. Median follow-up was 95.3 months. Cone beam CT image-guided EBRT consisted of 33 fractions of intensity-modulated radiation therapy with simultaneous integrated boost up to 76.23 Gy (DMean). Combined treatment was delivered as 46 Gy (DMean) EBRT, followed by two fractions HDR-BT boost with 9 Gy (D90%). Propensity score matching was applied before analysis of the primary endpoint, estimated 10-year biochemical relapse-free survival (bRFS), and the secondary endpoints metastasis-free survival (MFS) and overall survival (OS). Prognostic parameters were analyzed by Cox proportional hazard modelling. Genitourinary (GU)/gastrointestinal (GI) toxicity evaluation used the Common Toxicity Criteria for Adverse Events (v5.0).
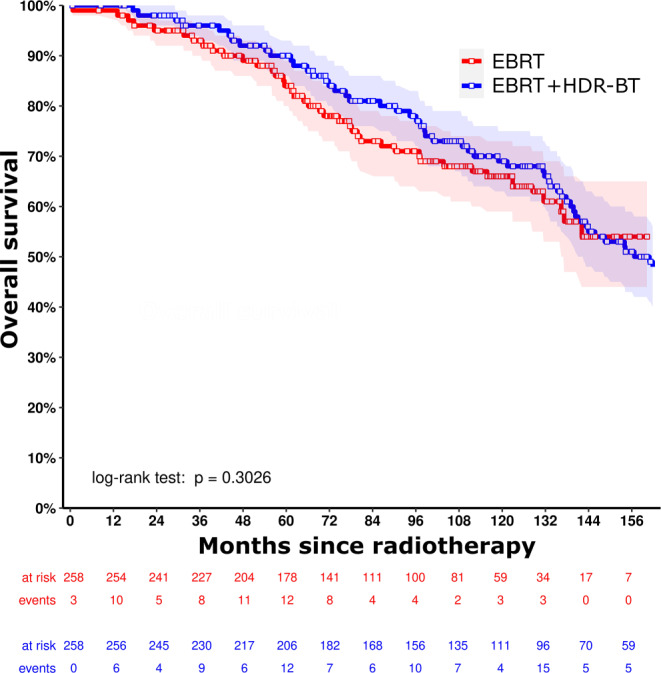
Results: The estimated 10-year bRFS was 82.0% vs. 76.4% (p = 0.075) for EBRT alone versus combined treatment, respectively. The estimated 10-year MFS was 82.9% vs. 87.0% (p = 0.195) and the 10-year OS was 65.7% vs. 68.9% (p = 0.303), respectively. Cumulative 5‑year late GU ≥ grade 2 toxicities were seen in 23.6% vs. 19.2% (p = 0.086) and 5‑year late GI ≥ grade 2 toxicities in 11.1% vs. 5.0% of the patients (p = 0.002); cumulative 5‑year late grade 3 GU toxicity occurred in 4.2% vs. 3.6% (p = 0.401) and GI toxicity in 1.0% vs. 0.3% (p = 0.249), respectively.
Conclusion: Both treatment groups showed excellent long-term outcomes with low rates of severe toxicity.
Keywords: Dose escalation; High-dose-rate brachytherapy boost; Long-term outcome; Propensity score matching; Toxicity.
© 2022. The Author(s).
Conflict of interest statement
J. Tamihardja, I. Lawrenz, P. Lutyj, S. Weick, M. Guckenberger, B. Polat, and M. Flentje declare that they have no competing interests.
Figures


Similar articles
-
Comparison of acute and late toxicities for three modern high-dose radiation treatment techniques for localized prostate cancer.Int J Radiat Oncol Biol Phys. 2012 Jan 1;82(1):204-12. doi: 10.1016/j.ijrobp.2010.10.009. Epub 2010 Dec 16. Int J Radiat Oncol Biol Phys. 2012. PMID: 21167653 Clinical Trial.
-
Two-Weekly High-Dose-Rate Brachytherapy Boost After External Beam Radiotherapy for Localized Prostate Cancer: Long-Term Outcome and Toxicity Analysis.Front Oncol. 2021 Nov 26;11:764536. doi: 10.3389/fonc.2021.764536. eCollection 2021. Front Oncol. 2021. PMID: 34900712 Free PMC article.
-
Comparing Iridium-192 with Cobalt-60 sources in high-dose-rate brachytherapy boost for localized prostate cancer.Acta Oncol. 2022 Jun;61(6):714-719. doi: 10.1080/0284186X.2022.2068968. Epub 2022 Apr 29. Acta Oncol. 2022. PMID: 35485446
-
Brachytherapy boost (BT-boost) or stereotactic body radiation therapy boost (SBRT-boost) for high-risk prostate cancer (HR-PCa).Cancer Radiother. 2021 Jun;25(4):400-409. doi: 10.1016/j.canrad.2020.11.004. Epub 2021 Jan 18. Cancer Radiother. 2021. PMID: 33478838
-
A Brief Review of Low-Dose Rate (LDR) and High-Dose Rate (HDR) Brachytherapy Boost for High-Risk Prostate.Front Oncol. 2019 Dec 10;9:1378. doi: 10.3389/fonc.2019.01378. eCollection 2019. Front Oncol. 2019. PMID: 31921640 Free PMC article. Review.
Cited by
-
Prostate brachytherapy boost: Long-term results of protocol-based treatment of patients with non-metastatic prostate cancer.J Contemp Brachytherapy. 2024 Dec;16(6):391-397. doi: 10.5114/jcb.2024.146671. Epub 2024 Dec 31. J Contemp Brachytherapy. 2024. PMID: 39943972 Free PMC article.
-
Biochemical control in intermediate- and high-risk prostate cancer after EBRT with and without brachytherapy boost.Strahlenther Onkol. 2025 Jan;201(1):11-19. doi: 10.1007/s00066-024-02245-3. Epub 2024 Jun 3. Strahlenther Onkol. 2025. PMID: 38829436 Free PMC article.
-
Comparison of chronic gastrointestinal and genitourinary toxicities between brachytherapy and external beam radiotherapy for patients with prostate cancer: A systematic review and meta-analysis.Technol Health Care. 2023;31(S1):357-372. doi: 10.3233/THC-236031. Technol Health Care. 2023. PMID: 37066936 Free PMC article.
-
Interactions between circRNAs and miR-141 in Cancer: From Pathogenesis to Diagnosis and Therapy.Int J Mol Sci. 2023 Jul 24;24(14):11861. doi: 10.3390/ijms241411861. Int J Mol Sci. 2023. PMID: 37511619 Free PMC article. Review.
References
-
- Al-Mamgani A, et al. Dose escalation and quality of life in patients with localized prostate cancer treated with radiotherapy: long-term results of the Dutch randomized dose-escalation trial (CKTO 96-10 trial) Int J Radiat Oncol Biol Phys. 2011;79(4):1004–1012. doi: 10.1016/j.ijrobp.2009.12.039. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
