

Double-level torsional osteotomy a treatment for the 'inwardly pointing knee' syndrome
- PMID: 35551448
- PMCID: PMC10191926
- DOI: 10.1007/s00402-022-04446-w
Double-level torsional osteotomy a treatment for the 'inwardly pointing knee' syndrome
Abstract
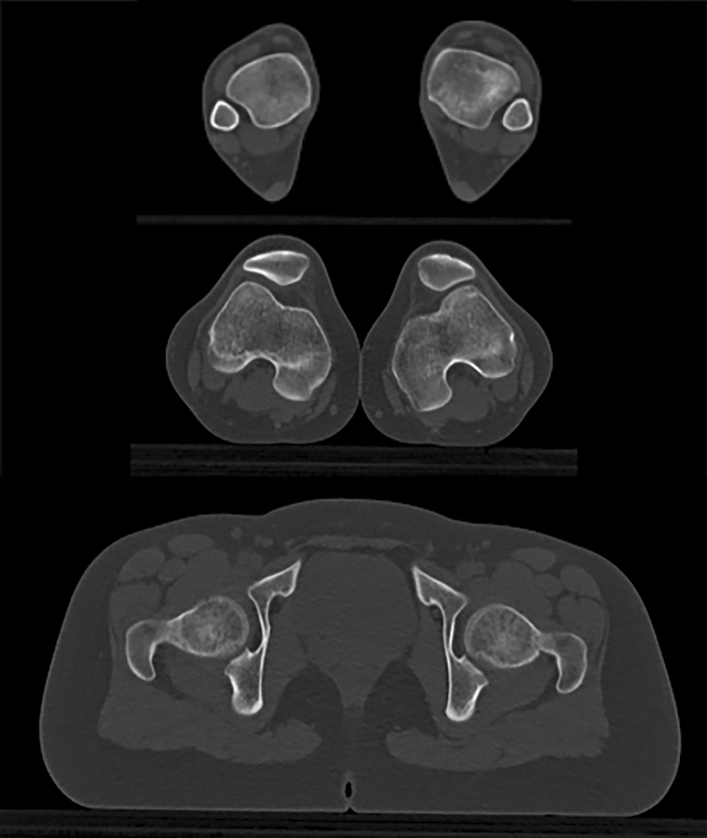
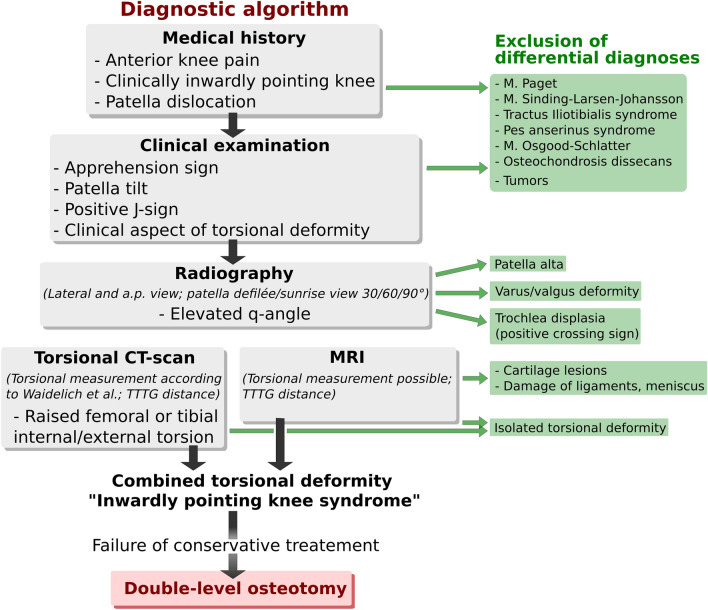
Introduction: A 'inwardly pointing knee' syndrome is a combined torsional deformity with increased femoral internal and tibial external torsion. After clinical and radiological verification of the torsional deformity and unsuccessful conservative therapy approach, a combined (double level) torsional osteotomy of femur and tibia might be the appropriate treatment. Here, we present the diagnostic algorithms, treatment, and outcome of combined torsional osteotomies of femur and tibia. The aim of the study is to show that patients treated with the procedure achieve patellofemoral stability and pain relief or reduction.
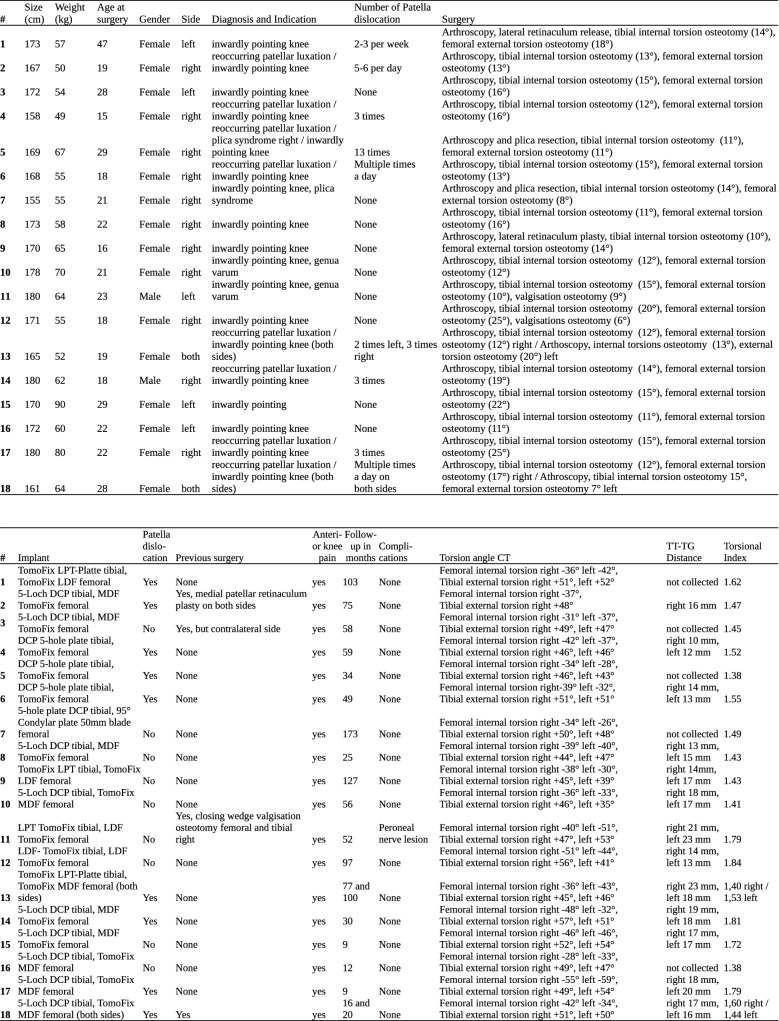
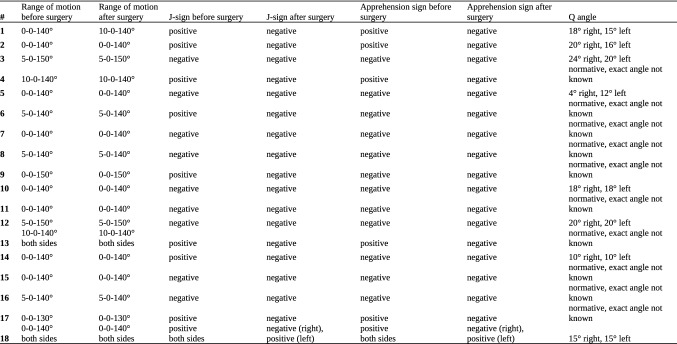
Material and methods: Twenty torsional osteotomies performed on 18 patients were included. Nine patients had experienced patellar dislocation in 11 joints before. All patients were suffering from anterior knee pain. All patients underwent a clinical and radiographical evaluation, including a torsion angle CT scan. Pre- and post-operatively multiple commonly approved scores (Lysholm Score, Tegner Activity score, Kujala Score, VAS and Japanese Knee Society score) were acquired.
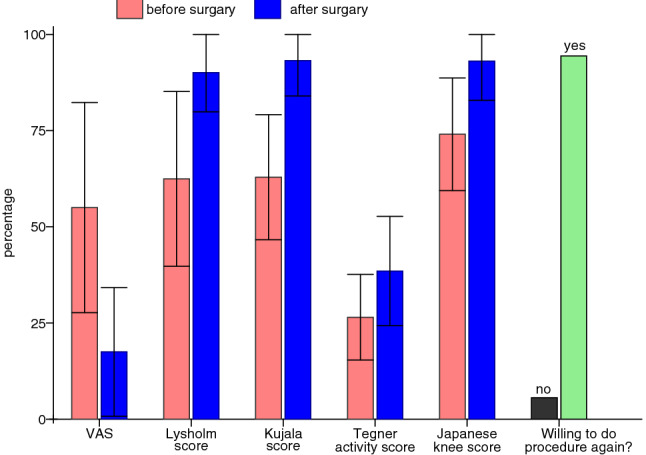
Results: In 18 patients we performed 20 double-level torsional osteotomies. 9 patients suffered from patellar dislocations in 11 knee joints prior to surgery. All patients were suffering from anterior knee pain. Of these 7 patients achieved a stable joint after surgery without further patellar dislocations. All achieved more knee stability and experienced less patellar luxation then before surgery. The mean duration of follow-up was 59 months (range 9-173 months). The mean VAS was significantly reduced by 3.75 points (SD 2.09, p value 0.0002) from 5.50 points (SD 2.73, range 0-9) before surgery to 1.75 points (SD 1.67, range 0-5) after surgery. The Lysholm score increased significantly by mean of 27.6 (SD 17.55, p value 0.0001) from mean 62.45 (SD 22.71, range 22-100) before surgery to mean 90.05 (SD 10.18, range 66-100) after surgery. The Kujala Score did improve significantly in average by 25.20 points (SD 13.61, p value 0.00012) from mean 62.9 (SD 16.24, range 35-95) to mean 93.2 (SD 9.20, range 66-100). The Tegner activity score did increase significantly by 1.2 points (SD 1.47, p value 0.004) in average from mean 2.65 (SD 1.11, range 1-5) to mean 3.85 (SD 1.42, range 1-6). The Japanese knee score did increase significantly by 19.15 in average (SD 11.95, p value 0.0001) from mean 74.05 (SD 14.63, range 33-95) to mean 93.05 (SD 10.18, range 68-100).
Conclusion: This is the first publication reporting about simultaneous double-level torsional osteotomies in a comparatively high number of patients. In addition, this is the first publication assessing the patient collective afterwards with objectifying clinical outcome scores. The results show that double-level torsional osteotomy is an effective treatment for patients with patellar dislocation or subluxation associated to torsional deformities of femur and tibia. Furthermore, we introduce a diagnostic algorithm for 'inwardly pointing knee' syndrome.
Level of evidence: Level IV.
Keywords: Anterior knee pain; Double level osteotomy; Inwardly pointing knee; Patellar dislocation; Patellofemoral instability; Torsional osteotomy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest. The conflict of interest declaration form has been signed by all authors.
Figures



Similar articles
-
Torsional osteotomies of the tibia in patellofemoral dysbalance.Arch Orthop Trauma Surg. 2017 Feb;137(2):179-185. doi: 10.1007/s00402-016-2599-1. Epub 2016 Dec 21. Arch Orthop Trauma Surg. 2017. PMID: 28004177
-
Clinical Results after Combined Distal Femoral Osteotomy in Patients with Patellar Maltracking and Recurrent Dislocations.J Knee Surg. 2019 Sep;32(9):924-933. doi: 10.1055/s-0038-1672125. Epub 2018 Oct 3. J Knee Surg. 2019. PMID: 30282099
-
Operative treatment of patellofemoral maltracking with torsional osteotomy.Arch Orthop Trauma Surg. 2012 Mar;132(3):289-98. doi: 10.1007/s00402-011-1303-8. Epub 2011 Apr 10. Arch Orthop Trauma Surg. 2012. PMID: 21479863
-
Tibial tubercle transfer leads to clinically relevant improvement in patients with patellar maltracking without instability: a systematic review and meta-analysis.Knee Surg Sports Traumatol Arthrosc. 2021 Apr;29(4):1137-1149. doi: 10.1007/s00167-020-06114-1. Epub 2020 Jun 27. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 32594329
-
Tibial derotational osteotomy for idiopathic tibial torsion: A systematic review of surgical indications based on clinical presentation and measurement technique.Knee Surg Sports Traumatol Arthrosc. 2024 Jul;32(7):1798-1809. doi: 10.1002/ksa.12231. Epub 2024 May 7. Knee Surg Sports Traumatol Arthrosc. 2024. PMID: 38713870
Cited by
-
[Tibial derotation osteotomy for knee joint pathologies : Indications, surgical technique and overview of the current literature].Orthopadie (Heidelb). 2025 Jul 14. doi: 10.1007/s00132-025-04675-y. Online ahead of print. Orthopadie (Heidelb). 2025. PMID: 40659923 Review. German.
-
Surgical management of miserable malalignment of the lower limb: a systematic review.Eur J Orthop Surg Traumatol. 2025 Jun 23;35(1):270. doi: 10.1007/s00590-025-04375-5. Eur J Orthop Surg Traumatol. 2025. PMID: 40548979 Review. No abstract available.
-
Intraoperative control by Schanz-screws is inaccurate to achieve the exact amount of correction in de-rotational osteotomies.Knee Surg Sports Traumatol Arthrosc. 2023 Oct;31(10):4319-4326. doi: 10.1007/s00167-023-07485-x. Epub 2023 Jun 17. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 37329368
-
Varus osteotomy as a salvage procedure for young patients with symptomatic patellofemoral arthritis and valgus malalignment at short- to mid-term follow-up: a case series.Arch Orthop Trauma Surg. 2024 Apr;144(4):1667-1673. doi: 10.1007/s00402-024-05212-w. Epub 2024 Feb 22. Arch Orthop Trauma Surg. 2024. PMID: 38386061 Free PMC article.
-
Complications after knee derotational osteotomies in patients with anterior knee pain and/or patellofemoral instability: a systematic review with meta-analysis.EFORT Open Rev. 2025 Jan 3;10(1):14-27. doi: 10.1530/EOR-2024-0036. Print 2025 Jan 1. EFORT Open Rev. 2025. PMID: 40071944 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
