Increase of Parkin and ATG5 plasmatic levels following perinatal hypoxic-ischemic encephalopathy
- PMID: 35551488
- PMCID: PMC9098891
- DOI: 10.1038/s41598-022-11870-w
Increase of Parkin and ATG5 plasmatic levels following perinatal hypoxic-ischemic encephalopathy
Abstract
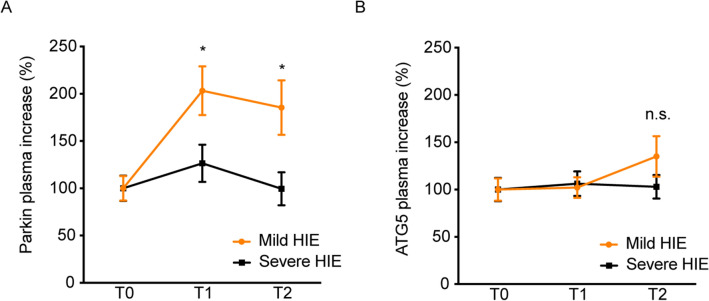
Brain injury at birth is an important cause of neurological and behavioral disorders. Hypoxic-ischemic encephalopathy (HIE) is a critical cerebral event occurring acutely or chronically at birth with high mortality and morbidity in newborns. Therapeutic strategies for the prevention of brain damage are still unknown, and the only medical intervention for newborns with moderate-to-severe HIE is therapeutic hypothermia (TH). Although the neurological outcome depends on the severity of the initial insult, emerging evidence suggests that infants with mild HIE who are not treated with TH have an increased risk for neurodevelopmental impairment; in the current clinical setting, there are no specific or validated biomarkers that can be used to both correlate the severity of the hypoxic insult at birth and monitor the trend in the insult over time. The aim of this work was to examine the presence of autophagic and mitophagic proteins in bodily fluids, to increase knowledge of what, early at birth, can inform therapeutic strategies in the first hours of life. This is a prospective multicentric study carried out from April 2019 to April 2020 in eight third-level neonatal intensive care units. All participants have been subjected to the plasma levels quantification of both Parkin (a protein involved in mitophagy) and ATG5 (involved in autophagy). These findings show that Parkin and ATG5 levels are related to hypoxic-ischemic insult and are reliable also at birth. These observations suggest a great potential diagnostic value for Parkin evaluation in the first 6 h of life.
Trial registration: ClinicalTrials.gov NCT03897101.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures