

Resection and reconstruction of huge tumors in the chest wall
- PMID: 35551615
- PMCID: PMC9097317
- DOI: 10.1186/s13019-022-01877-9
Resection and reconstruction of huge tumors in the chest wall
Abstract
Objective: To evaluate the experience and effects of resection and reconstruction of 4 cases of huge tumors in the chest wall.
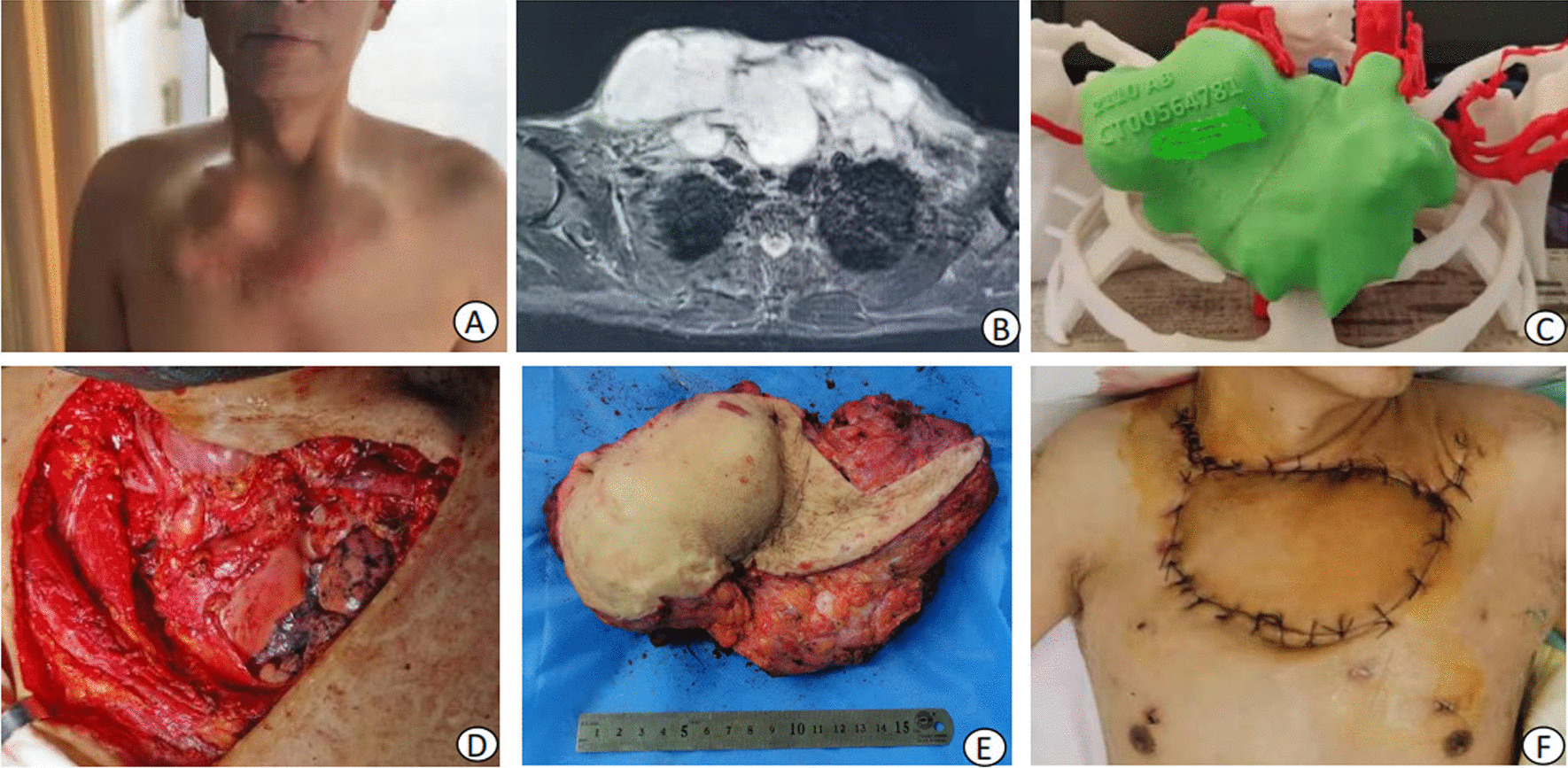
Methods: The clinical data of 4 patients with huge tumors in the chest wall from July 2015 to January 2020 were collected and analyzed. There were 2 males and 2 females.Chondrosarcoma was diagnosed in 2 cases, giant cell tumor was diagnosed in 1 case,and metastasis from breast cancer was diagnosed in 1 case.All patients underwent extensive tumor resection and had thoracic exposure after tumor resection.Two patients underwent reconstruction with mesh and titanium mesh, and the incision was closed directly.The third patient underwent reconstruction with mesh and latissimus dorsi flap,and the fourth patient underwent reconstruction with mesh,titanium mesh and latissimus dorsi flap.
Result: One patient had incision infection after operation,which resolved after debridement.All patients were followed up for 2-6 years, no tumor recurrence or metastasis was noted during follow-up.None of patients had abnormal breathing, dyspnea or other physical discomfort.
Conclusion: It is difficult to resect the huge tumors in the chest wall,and it is more reasonable and safer to choose a reconstruction method using mesh and titanium mesh.The latissimus dorsi flap can achieve good results in repairing soft tissue defects.Close perioperative management and multidisciplinary team discussions can help to achieve better curative effects.
Keywords: Chest wall tumor; Multidisciplinary; Perioperative period; Reconstruction; Resection.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
