

Integrated care for optimizing the management of stroke and associated heart disease: a position paper of the European Society of Cardiology Council on Stroke
- PMID: 35552401
- PMCID: PMC9259378
- DOI: 10.1093/eurheartj/ehac245
Integrated care for optimizing the management of stroke and associated heart disease: a position paper of the European Society of Cardiology Council on Stroke
Abstract
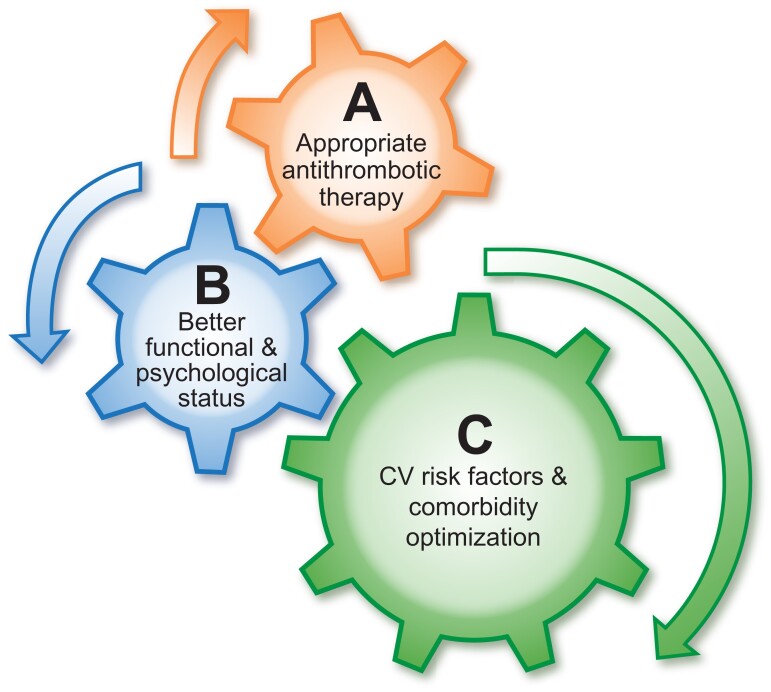
The management of patients with stroke is often multidisciplinary, involving various specialties and healthcare professionals. Given the common shared risk factors for stroke and cardiovascular disease, input may also be required from the cardiovascular teams, as well as patient caregivers and next-of-kin. Ultimately, the patient is central to all this, requiring a coordinated and uniform approach to the priorities of post-stroke management, which can be consistently implemented by different multidisciplinary healthcare professionals, as part of the patient 'journey' or 'patient pathway,' supported by appropriate education and tele-medicine approaches. All these aspects would ultimately aid delivery of care and improve patient (and caregiver) engagement and empowerment. Given the need to address the multidisciplinary approach to holistic or integrated care of patients with heart disease and stroke, the European Society of Cardiology Council on Stroke convened a Task Force, with the remit to propose a consensus on Integrated care management for optimizing the management of stroke and associated heart disease. The present position paper summarizes the available evidence and proposes consensus statements that may help to define evidence gaps and simple practical approaches to assist in everyday clinical practice. A post-stroke ABC pathway is proposed, as a more holistic approach to integrated stroke care, would include three pillars of management: A: Appropriate Antithrombotic therapy.B: Better functional and psychological status.C: Cardiovascular risk factors and Comorbidity optimization (including lifestyle changes).
Keywords: Delivery of care; Heart disease; Integrated care; Patient pathways; Stroke.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures
References
-
- Fischer U, de Sousa D A, Norrving B, Caso V. Status and perspectives of acute stroke care in Europe. Stroke 2018;49:2281–2282. - PubMed
-
- Lip GYH. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol 2017;14:627–628. - PubMed
-
- Field M, Kuduvalli M, Torella F, McKay V, Khalatbari A, Lip GY. Integrated care pathways and the aortovascular hub. Thromb Haemost 2022;122(2):177–180. - PubMed
-
- Moudallel S, van den Bemt BJF, Zwikker H, de Veer A, Rydant S, Dijk LV, et al. Association of conflicting information from healthcare providers and poor shared decision making with suboptimal adherence in direct oral anticoagulant treatment: a cross-sectional study in patients with atrial fibrillation. Patient Educ Couns 2021;104:155–162. - PubMed
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J 2021;42(5):373–498. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
