

Functional in-vitro evaluation of the non-specific effects of BCG vaccination in a randomised controlled clinical study
- PMID: 35552463
- PMCID: PMC9096342
- DOI: 10.1038/s41598-022-11748-x
Functional in-vitro evaluation of the non-specific effects of BCG vaccination in a randomised controlled clinical study
Abstract
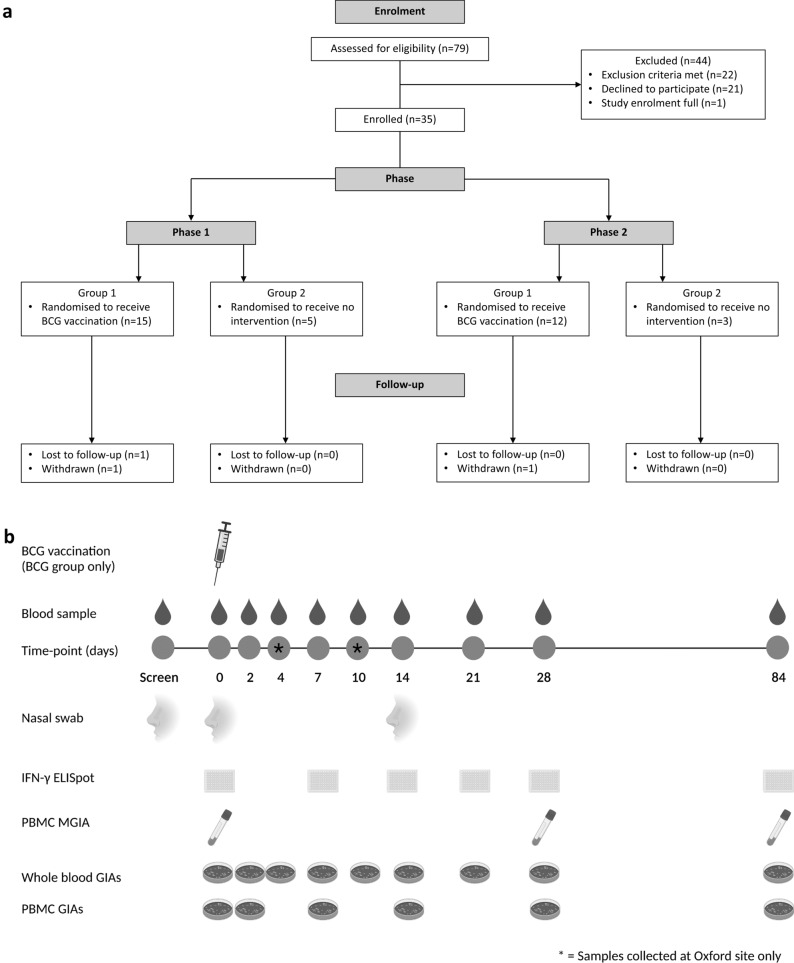
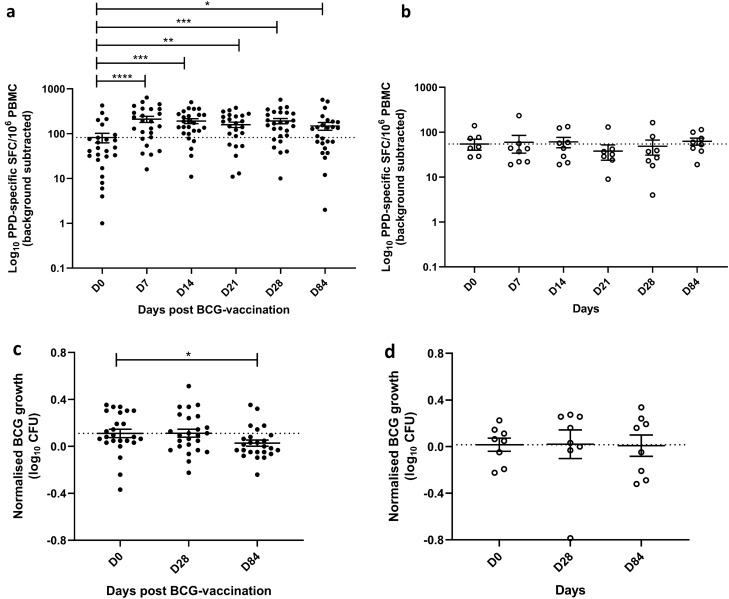
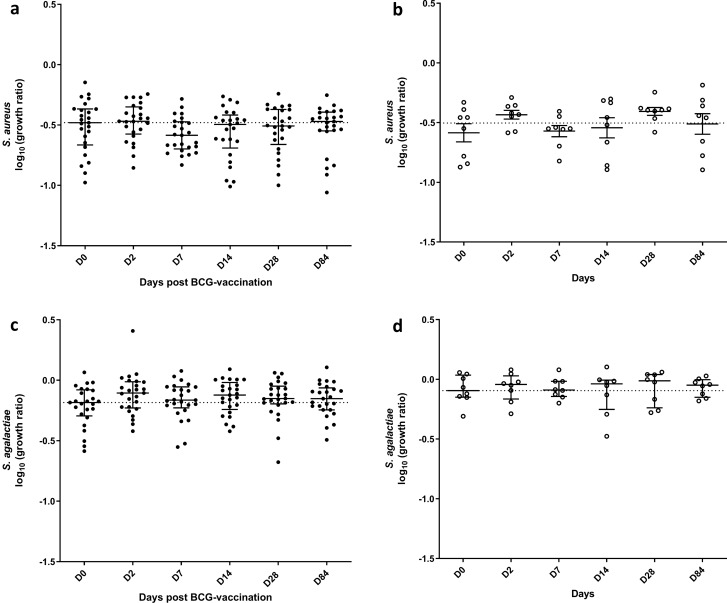
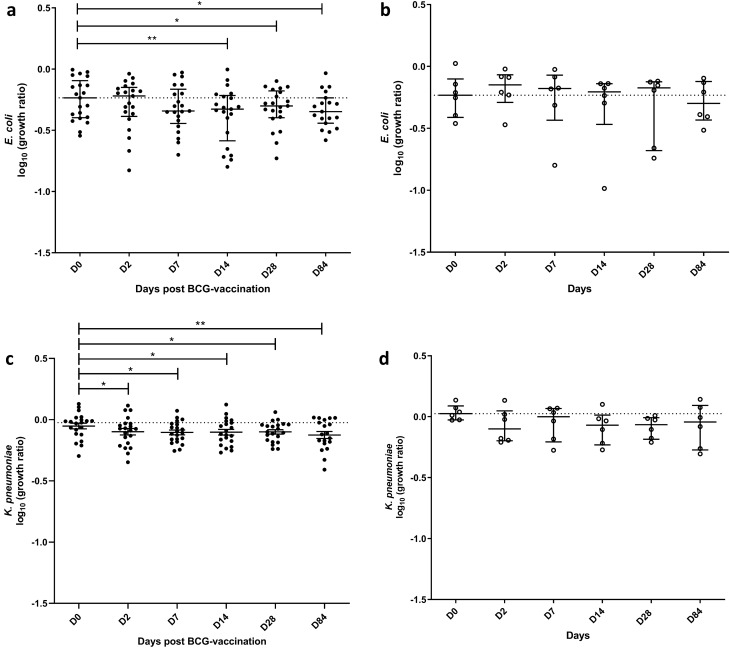
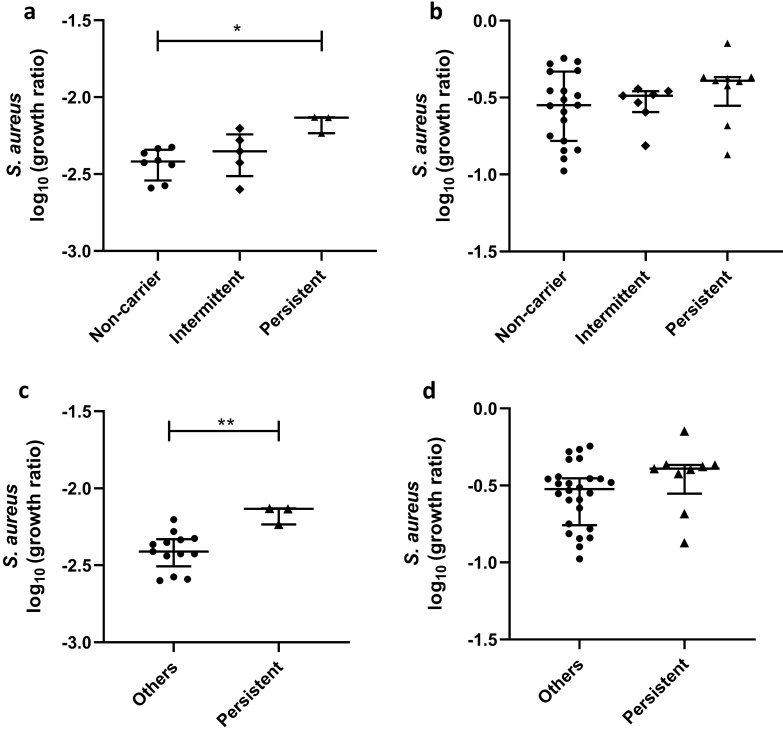
Bacille Calmette-Guérin (BCG), the only currently licenced tuberculosis vaccine, may exert beneficial non-specific effects (NSE) in reducing infant mortality. We conducted a randomised controlled clinical study in healthy UK adults to evaluate potential NSE using functional in-vitro growth inhibition assays (GIAs) as a surrogate of protection from four bacteria implicated in infant mortality. Volunteers were randomised to receive BCG intradermally (n = 27) or to be unvaccinated (n = 8) and were followed up for 84 days; laboratory staff were blinded until completion of the final visit. Using GIAs based on peripheral blood mononuclear cells, we observed a significant reduction in the growth of the Gram-negative bacteria Escherichia coli and Klebsiella pneumonia following BCG vaccination, but no effect for the Gram-positive bacteria Staphylococcus aureus and Streptococcus agalactiae. There was a modest association between S. aureus nasal carriage and growth of S. aureus in the GIA. Our findings support a causal link between BCG vaccination and improved ability to control growth of heterologous bacteria. Unbiased assays such as GIAs are potentially useful tools for the assessment of non-specific as well as specific effects of TB vaccines. This study was funded by the Bill and Melinda Gates Foundation and registered with ClinicalTrials.gov (NCT02380508, 05/03/2015; completed).
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
