

The healthy female microbiome across body sites: effect of hormonal contraceptives and the menstrual cycle
- PMID: 35553675
- PMCID: PMC9247429
- DOI: 10.1093/humrep/deac094
The healthy female microbiome across body sites: effect of hormonal contraceptives and the menstrual cycle
Abstract
Study question: How does hormonal contraceptive use and menstrual cycle phase affect the female microbiome across different body sites?
Summary answer: The menstrual cycle phase, but not hormonal contraceptive use, is associated with the vaginal and oral but not the gut microbiome composition in healthy young women.
What is known already: Women with low vaginal levels of Lactobacillus crispatus are at increased risk of pre-term birth, fertility treatment failure, sexually transmitted infections and gynaecological cancers. Little is known about the effect of hormonal fluctuations on other body site's microbiomes as well as the interplay between them.
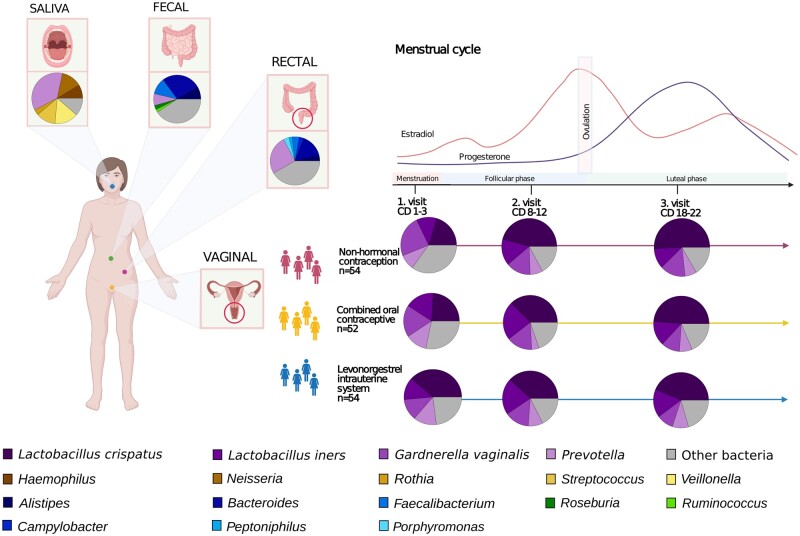
Study design, size, duration: This study includes a cohort of 160 healthy young Danish women using three different contraceptive regimens: non-hormonal methods (n = 54), combined oral contraceptive (COC, n = 52) or levonorgestrel intrauterine system (LNG-IUS, n = 54). Samples were collected from four body sites during the menstrual cycle (menses, follicular and luteal phases) at Copenhagen University Hospital, Rigshospitalet, Denmark.
Participants/materials, setting, methods: The oral, vaginal, rectal and faecal microbiomes were characterized by shotgun sequencing. Microbial diversity and community distance measures were compared between study groups, menstrual phase timepoints and body sites. All participants answered an extensive questionnaire on current health, lifestyle and sex life. Confounding factors such as smoking, BMI and diet were analysed by PERMANOVA. Plasma oestradiol and progesterone levels are correlated with microbiome composition.
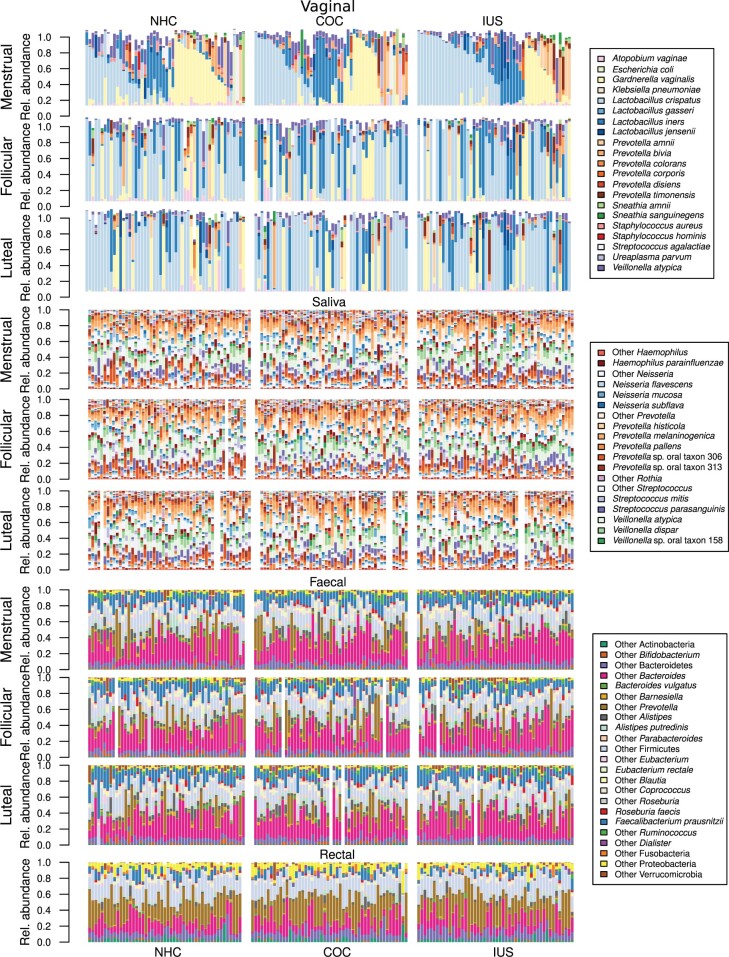
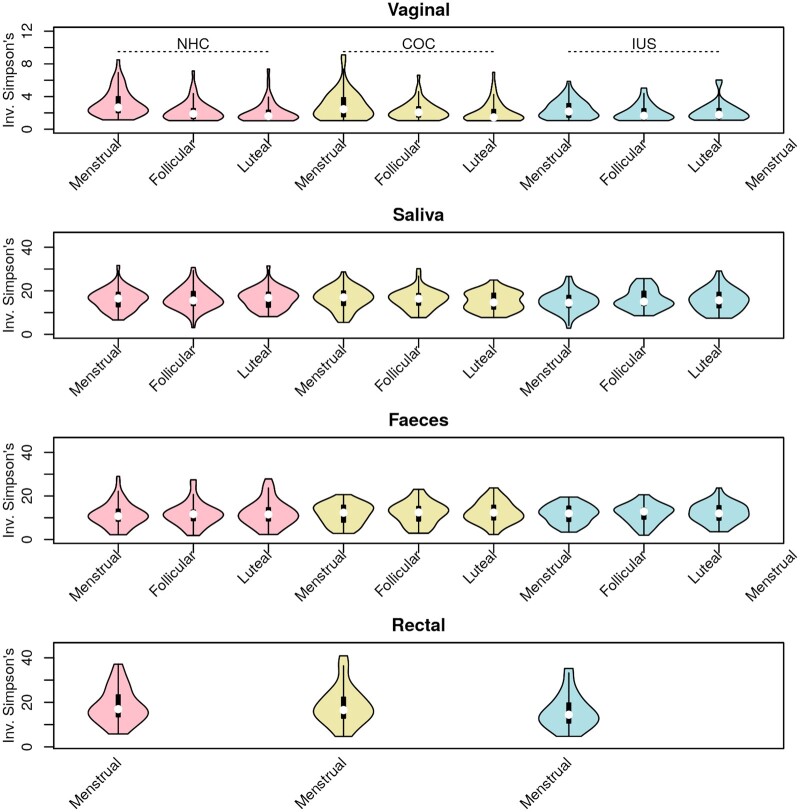
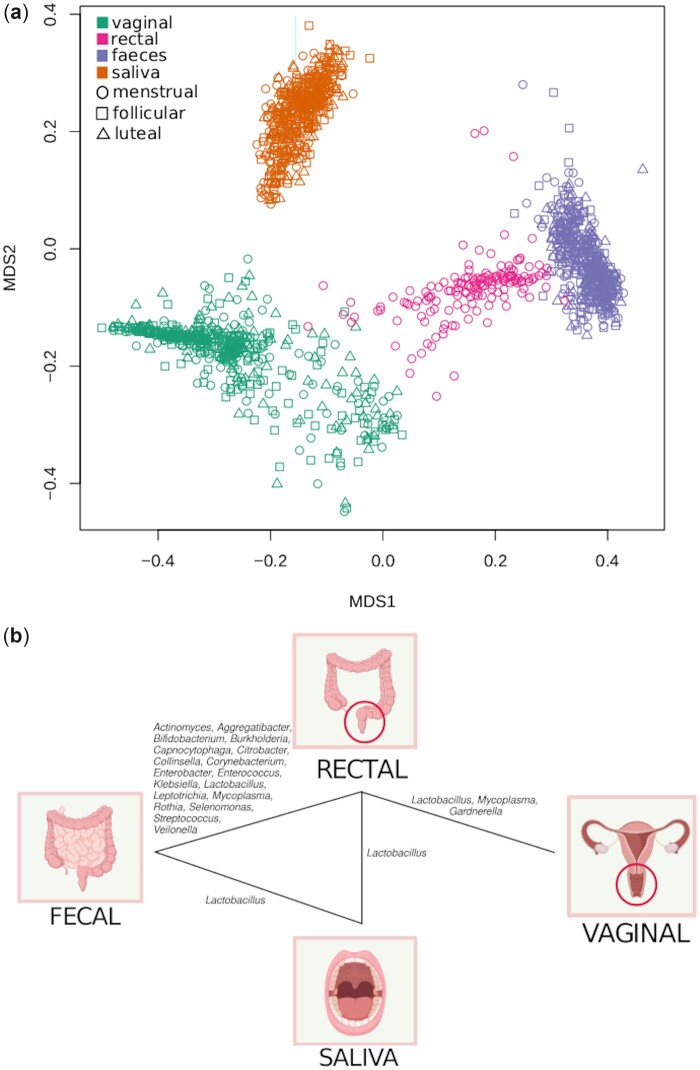
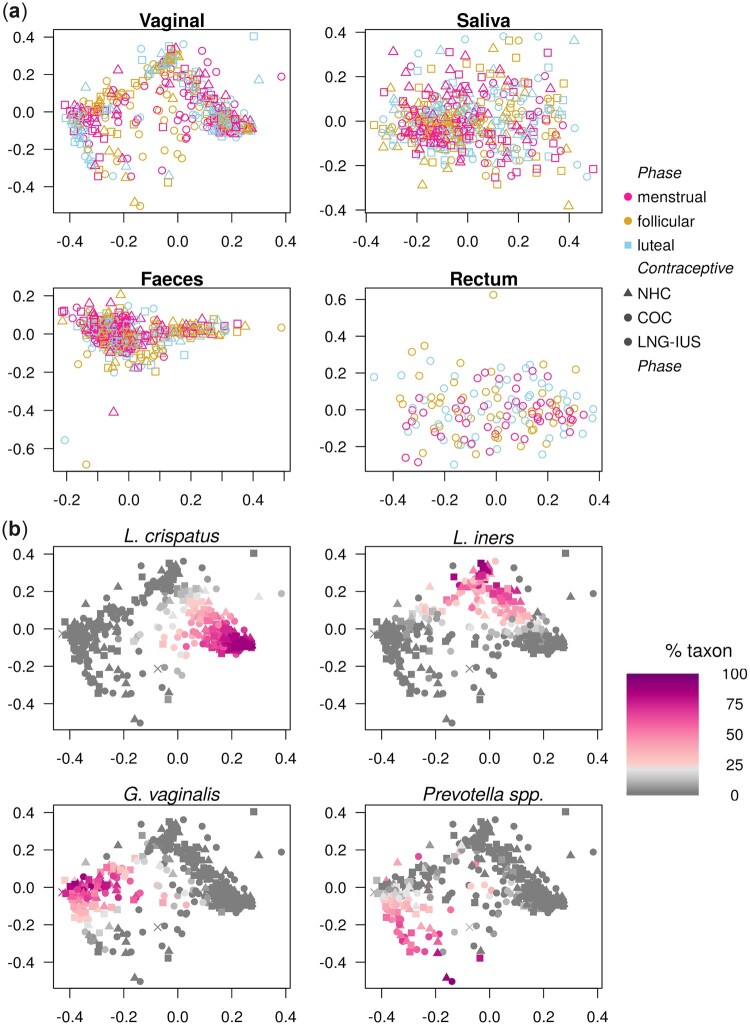
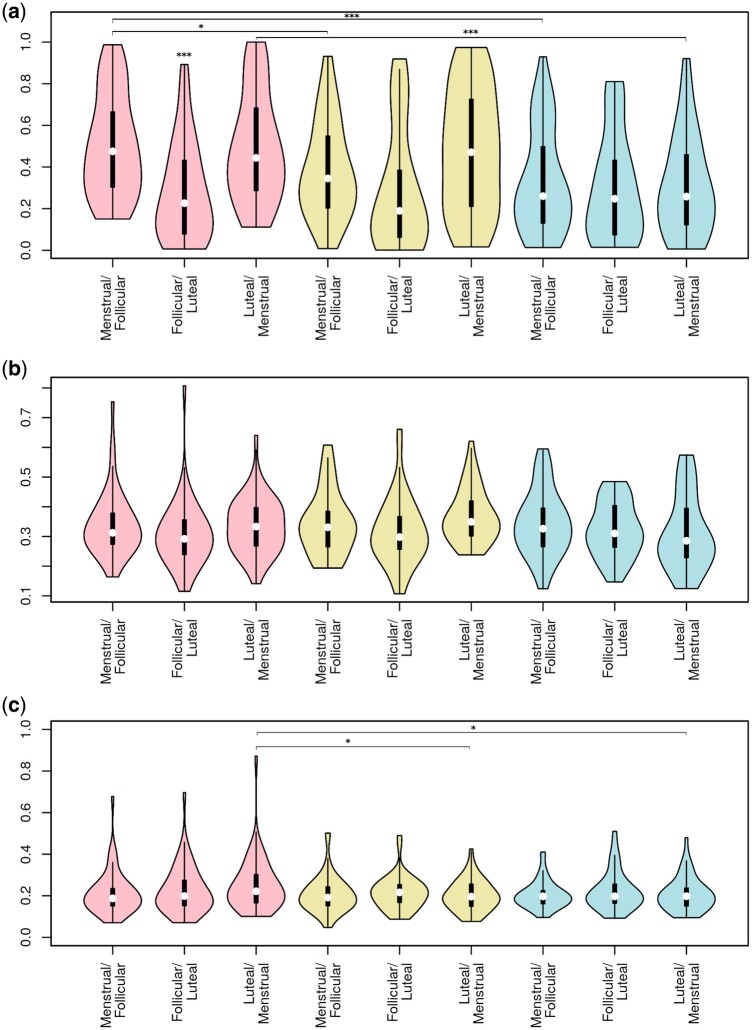
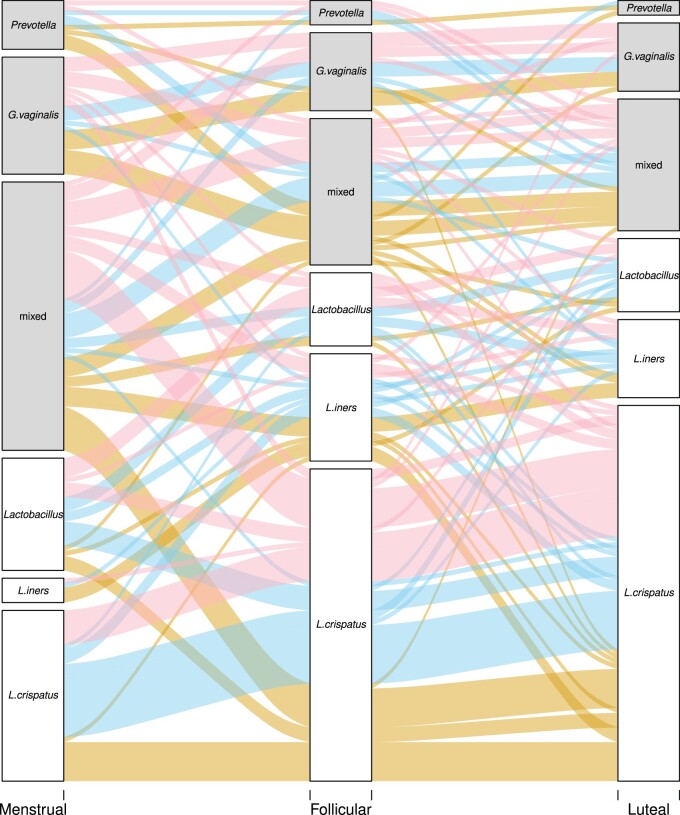
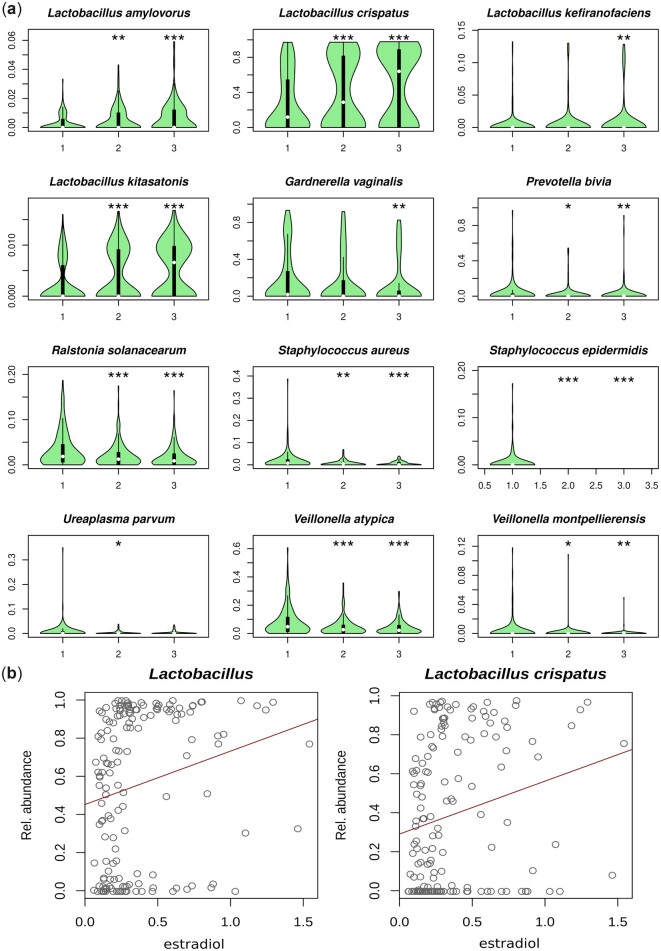
Main results and the role of chance: The use of COC and LNG-IUS was not associated with the microbiome composition or diversity. However, increased diversity in the vaginal microbiome was observed during menses, followed by a subsequent expansion of Lactobacillus spp. during the follicular and luteal phases which correlated with measured serum oestradiol levels (r = 0.11, P < 0.001). During menses, 89 women (58%) had a dysbiotic vaginal microbiome with <60% Lactobacillus spp. This declined to 49 (32%) in the follicular phase (P < 0.001) and 44 (29%) in the luteal phase (P < 0.001). During menses, bacterial richness and diversity in saliva reached its lowest point while no differences were observed in the faecal microbiome. The microbiome in different body sites was on average more similar within the same individual than between individuals, despite phase or hormonal treatment. Only the vagina presented a clear cluster structure with dominance of either L. crispatus, Lactobacillus iners, Gardnerella vaginalis or Prevotella spp.
Large scale data: The microbiome samples analysed in this study were submitted to the European Nucleotide Archive under project number PRJEB37731, samples ERS4421369-ERS4422941.
Limitations, reasons for caution: The cohort is homogenous which limits extrapolation of the effects of ethnicity and socio-economic status on the microbiome. We only present three defined timepoints across the menstrual phase and miss potential important day to day fluctuations.
Wider implications of the findings: The use of hormonal contraception did not significantly associate with the microbiome composition in the vagina, faeces, rectum or saliva in healthy young women. This is a welcome finding considering the widespread and prolonged use of these highly efficient contraceptive methods. The menstrual cycle is, however, a major confounding factor for the vaginal microbiome. As such, the time point in the menstrual cycle should be considered when analysing the microbiome of women of reproductive age, since stratifying by vaginal dysbiosis status during menstruation could be misleading. This is the first study to confirm by direct measurements of oestradiol, a correlation with the presence of L. crispatus, adding evidence of a possible hormonal mechanism for the maintenance of this desirable microbe.
Study funding/competing interest(s): This work was partly funded by the Ferring Pharmaceuticals through a research collaboration with The Centre for Translational Microbiome Research (CTMR) at the Karolinska Institutet (L.W.H., E.F., G.E. and I.S.-K.). Ferring Pharmaceuticals also funded the infrastructure to obtain the clinical samples at Copenhagen University Hospital ([#MiHSN01], M.C.K., Z.B., and H.S.N.). This work was also supported by funding from Rigshospitalet's Research Funds ([#E-22614-01 and #E-22614-02] to M.C.K.) and Oda and Hans Svenningsen's Foundation ([#F-22614-08] to H.S.N.). M.C.K., L.W.H., E.F., Z.B., G.E., L.E., I.S.-K. and H.S.N., are partially funded by Ferring Pharmaceuticals, which also provided funds for the collection and processing of the samples analysed in this study. H.S.N.'s research is further supported by Freya Biosciences and the BioInnovation Institute. H.S.N. has received honoraria from Ferring Pharmaceuticals, Merck A/S, Astra-Zeneca, Cook Medical and Ibsa Nordic. A.N.A. reports no competing interests.
Keywords: hormonal contraceptives; menstrual cycle; microbiome; shotgun sequencing; womens reproductive health.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Figures
References
-
- Antonio MAD, Rabe LK, Hillier SL.. Colonization of the rectum by Lactobacillus species and decreased risk of bacterial vaginosis. J Infect Dis 2005;192:394–398. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
