

Efficacy of Bariatric Surgery in the Treatment of Women With Obesity and Polycystic Ovary Syndrome
- PMID: 35554540
- PMCID: PMC9282367
- DOI: 10.1210/clinem/dgac294
Efficacy of Bariatric Surgery in the Treatment of Women With Obesity and Polycystic Ovary Syndrome
Abstract
Context: The comparative effectiveness of drugs and surgical therapy for women with obesity and polycystic ovary syndrome (PCOS) has not been systematically compared.
Objective: We aimed to determine the difference in efficacy between drug and bariatric surgery therapy for women with obesity and PCOS.
Methods: This prospective nonrandomized trial enrolled 90 women aged 18 to 40 years with body mass index (BMI) ≥ 27.5 kg/m2 and waist circumference ≥ 85 cm and fulfilling the 2011 Chinese diagnostic criteria for PCOS; 81 subjects completed the study. In the drug group, patients were administered metformin and an oral contraceptive containing ethinyl-estradiol and cyproterone acetate for the first 6 months, and metformin alone for the second 6 months. In the surgical group, patients underwent laparoscopic sleeve gastrectomies. The follow-up period was 12 months. The main outcome was the complete remission of PCOS, requiring 6 consecutive regular menstruation cycles or spontaneous pregnancy.
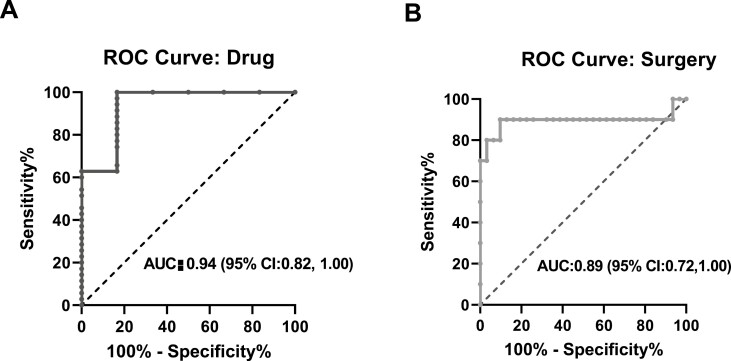
Results: Median BMI at endpoint was 30.1 kg/m2 in the drug group and 23.7 kg/m2 in the surgical group; complete remission rate was 15% and 78%, respectively. Except endpoint BMI, no difference was observed in free androgen index, ovarian morphology, homeostasis model assessment for insulin resistance, and total weight loss between remission and nonremission patients. Logistic regression analyses also revealed that the final BMI was the major factor influencing the remission of PCOS. The cutoff points for the final BMI were 27.5 kg/m2 for the drug group and 26 kg/m2 for the surgical group. Overall, nearly 95% of patients with an endpoint BMI below the cutoff values achieved complete remission.
Conclusion: Complete remission of PCOS in patients with obesity depends on the final BMI after weight loss. Thus, bariatric surgery should be prioritized for these patients.
Keywords: TWL; bariatric surgery; obesity; polycystic ovary syndrome; weight loss.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures




References
-
- Balen AH, Morley LC, Misso M, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update. 2016;22(6):687-708. - PubMed
-
- Walters KA, Gilchrist RB, Ledger WL, Teede HJ, Handelsman DJ, Campbell RE. New perspectives on the pathogenesis of PCOS: neuroendocrine origins. Trends Endocrinol Metab. 2018;29(12):841-852. - PubMed
-
- Patel S. Polycystic ovary syndrome (PCOS), an inflammatory, systemic, lifestyle endocrinopathy. J Steroid Biochem Mol Biol. 2018;182:27-36. - PubMed
-
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 194: polycystic ovary syndrome. Obstet Gynecol. 2018;131(6):e157-e171. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
