

Comparison of a preoperative MR-based recurrence risk score versus the postoperative score and four clinical staging systems in hepatocellular carcinoma: a retrospective cohort study
- PMID: 35554652
- PMCID: PMC9668764
- DOI: 10.1007/s00330-022-08811-6
Comparison of a preoperative MR-based recurrence risk score versus the postoperative score and four clinical staging systems in hepatocellular carcinoma: a retrospective cohort study
Abstract
Objectives: To establish a risk score integrating preoperative gadoxetic acid-enhanced magnetic resonance imaging (EOB-MRI) and clinical parameters to predict recurrence after hepatectomy for patients with hepatocellular carcinoma (HCC) and to compare its performance with that of a postoperative score and four clinical staging systems.
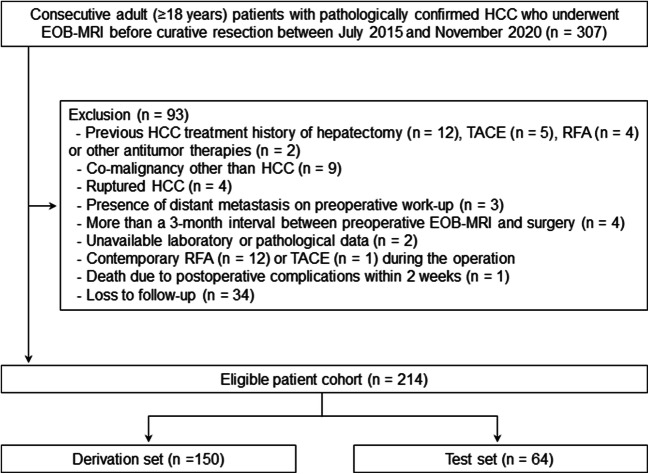
Methods: Consecutive patients with surgically confirmed HCC who underwent preoperative EOB-MRI between July 2015 and November 2020 were retrospectively included. Two recurrence risk scores, one incorporating only preoperative variables and the other incorporating all preoperative and postoperative variables, were constructed via Cox regression models.
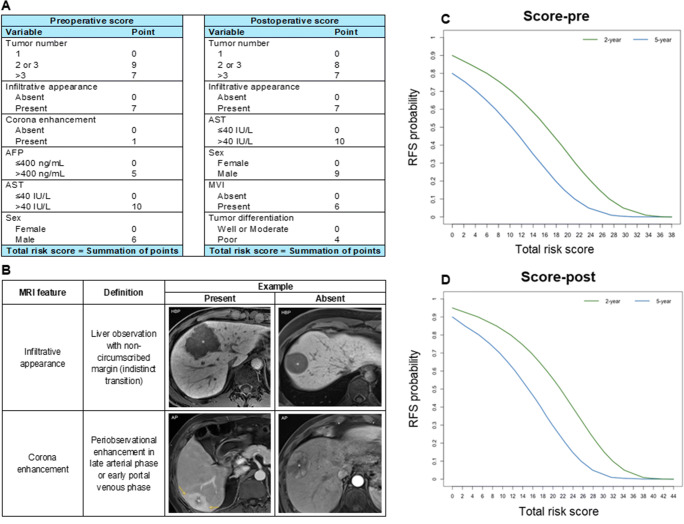
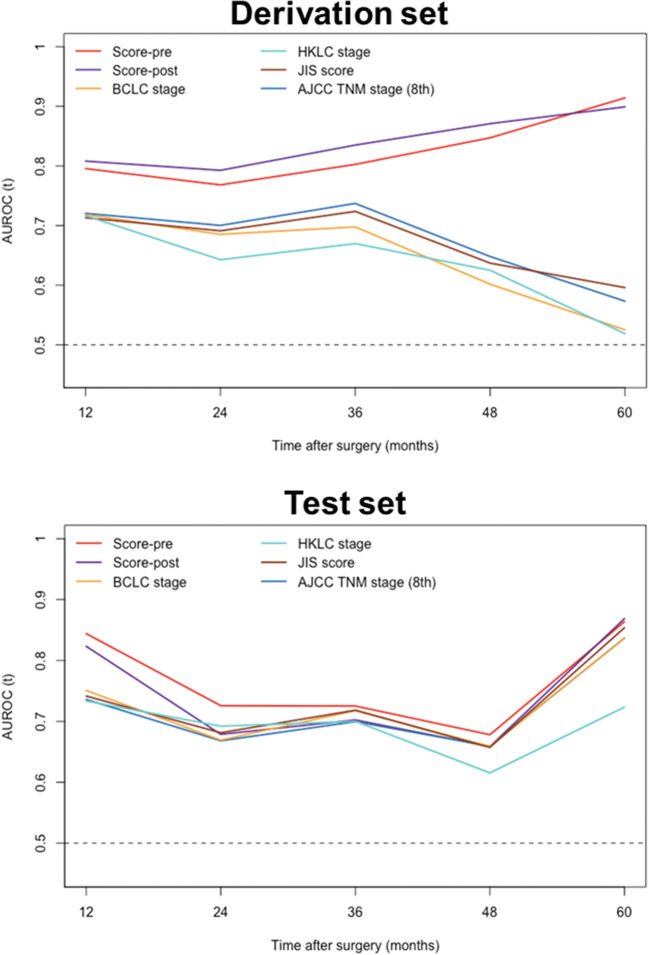
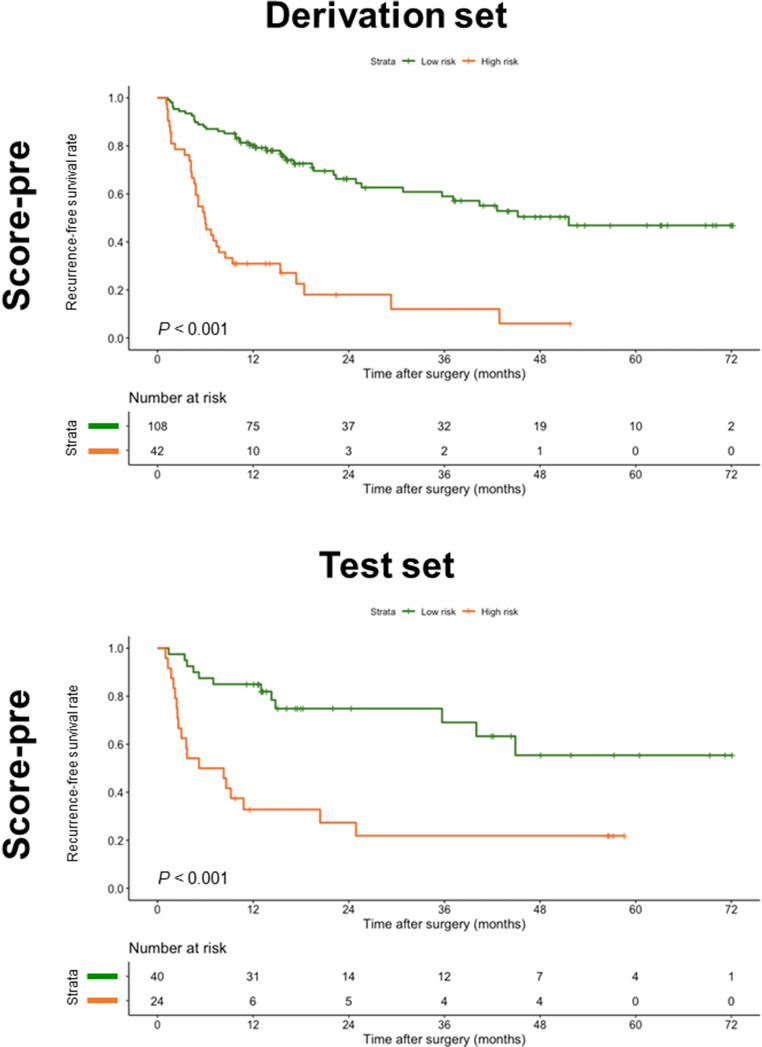
Results: A total of 214 patients (derivation set, n = 150; test set, n = 64) were included. Six preoperative variables, namely tumor number, infiltrative appearance, corona enhancement, alpha-fetoprotein (AFP) level, aspartate aminotransferase (AST) level, and sex, were independently associated with recurrence. After adding postoperative features, microvascular invasion and tumor differentiation were additional significant variables in lieu of corona enhancement and AFP level. Using the above variables, the preoperative score achieved a C-index of 0.741 on the test set, which was comparable with that of the postoperative score (0.729; p = 0.235). The preoperative score yielded a larger time-dependent area under the receiver operating characteristic curve at 1 year (0.844) than three existing systems (0.734-0.742; p < 0.05 for all). Furthermore, the preoperative score stratified patients into two prognostically distinct risk strata with low and high risks of recurrence (p < 0.001).
Conclusion: The preoperative score integrating EOB-MRI features, AFP and AST levels, and sex improves recurrence risk estimation in HCC.
Key points: • The preoperative risk score incorporating three EOB-MRI findings, AFP and AST levels, and sex achieved comparable performance with that of the postoperative score for predicting recurrence after hepatectomy in patients with HCC. • Two risk strata with low and high risks of recurrence were obtained based on the preoperative score. • The preoperative score may help tailor pretreatment decision-making and facilitate candidate selection for adjuvant clinical trials.
Keywords: Carcinoma, hepatocellular; Gadolinium ethoxybenzyl DTPA; Hepatectomy; Magnetic resonance imaging; Recurrence.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
Similar articles
-
Preoperative and postoperative MRI-based models versus clinical staging systems for predicting early recurrence in hepatocellular carcinoma.Eur J Surg Oncol. 2024 Sep;50(9):108476. doi: 10.1016/j.ejso.2024.108476. Epub 2024 Jun 8. Eur J Surg Oncol. 2024. PMID: 38870875
-
Deep learning nomogram based on Gd-EOB-DTPA MRI for predicting early recurrence in hepatocellular carcinoma after hepatectomy.Eur Radiol. 2023 Jul;33(7):4949-4961. doi: 10.1007/s00330-023-09419-0. Epub 2023 Feb 14. Eur Radiol. 2023. PMID: 36786905 Free PMC article.
-
Preoperative prediction of glypican-3 positive expression in solitary hepatocellular carcinoma on gadoxetate-disodium enhanced magnetic resonance imaging.Front Immunol. 2022 Aug 25;13:973153. doi: 10.3389/fimmu.2022.973153. eCollection 2022. Front Immunol. 2022. PMID: 36091074 Free PMC article.
-
Application of Gd-EOB-DTPA-enhanced magnetic resonance imaging (MRI) in hepatocellular carcinoma.World J Surg Oncol. 2020 Aug 22;18(1):219. doi: 10.1186/s12957-020-01996-4. World J Surg Oncol. 2020. PMID: 32828123 Free PMC article. Review.
-
Hepatobiliary phase hypointense nodule without arterial phase hyperenhancement: are they at risk of HCC recurrence after ablation or surgery? A systematic review and meta-analysis.Eur Radiol. 2020 Mar;30(3):1624-1633. doi: 10.1007/s00330-019-06499-9. Epub 2019 Nov 27. Eur Radiol. 2020. PMID: 31776747
Cited by
-
Ensemble learning based on efficient features combination can predict the outcome of recurrence-free survival in patients with hepatocellular carcinoma within three years after surgery.Front Oncol. 2022 Nov 10;12:1019009. doi: 10.3389/fonc.2022.1019009. eCollection 2022. Front Oncol. 2022. PMID: 36439437 Free PMC article.
-
Nomograms established for predicting microvascular invasion and early recurrence in patients with small hepatocellular carcinoma.BMC Cancer. 2024 Aug 1;24(1):929. doi: 10.1186/s12885-024-12655-2. BMC Cancer. 2024. PMID: 39090609 Free PMC article.
-
Multimodal imaging-based prediction of recurrence for unresectable HCC after downstage and resection-cohort study.Int J Surg. 2024 Sep 1;110(9):5672-5684. doi: 10.1097/JS9.0000000000001752. Int J Surg. 2024. PMID: 38833331 Free PMC article.
-
Risk stratification of solitary hepatocellular carcinoma ≤ 5 cm without microvascular invasion: prognostic values of MR imaging features based on LI-RADS and clinical parameters.Eur Radiol. 2023 May;33(5):3592-3603. doi: 10.1007/s00330-023-09484-5. Epub 2023 Mar 8. Eur Radiol. 2023. PMID: 36884087
-
MRI radiomics based on deep learning automated segmentation to predict early recurrence of hepatocellular carcinoma.Insights Imaging. 2024 May 20;15(1):120. doi: 10.1186/s13244-024-01679-8. Insights Imaging. 2024. PMID: 38763975 Free PMC article.
References
MeSH terms
Substances
Grants and funding
- No. 81971571/National Natural Science Foundation of China
- No. 82101997/National Natural Science Foundation of China
- No. 81901700/National Natural Science Foundation of China
- No. 2021YFS0141/Science and Technology Support Program of Sichuan Province
- No. 2021YFS0021/Science and Technology Support Program of Sichuan Province
LinkOut - more resources
Full Text Sources
Medical
