

Insights on Distinct Left Atrial Remodeling Between Atrial Fibrillation and Heart Failure With Preserved Ejection Fraction
- PMID: 35557544
- PMCID: PMC9086706
- DOI: 10.3389/fcvm.2022.857360
Insights on Distinct Left Atrial Remodeling Between Atrial Fibrillation and Heart Failure With Preserved Ejection Fraction
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) and atrial fibrillation (AF) commonly coexist with overlapping pathophysiology like left atrial (LA) remodeling, which might differ given different underlying mechanisms.
Objectives: We sought to investigate the different patterns of LA wall remodeling in AF vs. HFpEF.
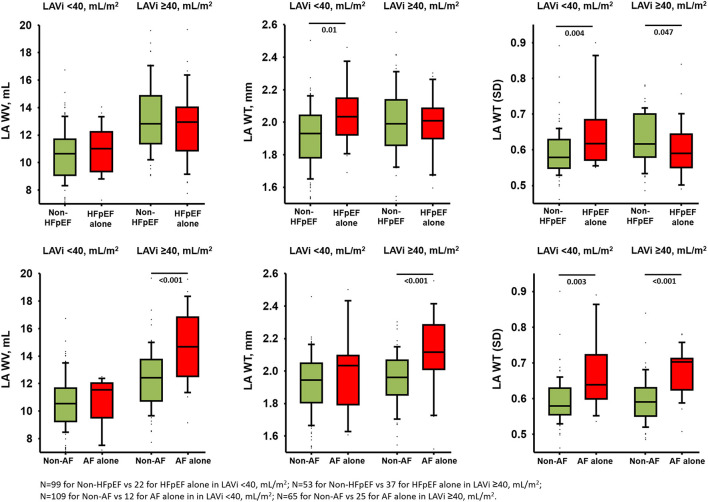
Methods: We compared LA wall characteristics including wall volume (LAWV), wall thickness (LAWT), and wall thickness heterogeneity (LAWT[SD]) and LA structure, function among the controls (without AF or HFpEF, n = 115), HFpEF alone (n = 59), AF alone (n = 37), and HFpEF+AF (n = 38) groups using multi-detector computed tomography and echocardiography.
Results: LA wall remodeling was most predominant and peak atrial longitudinal strain (PALS) was worst in HFpEF+AF patients as compared to the rest. Despite lower E/e' (9.8 ± 3.8 vs. 13.4 ± 6.4) yet comparable LA volume, LAWT and PALS in AF alone vs. HFpEF alone, LAWV [12.6 (11.6-15.3) vs. 12.0 (10.2-13.7); p = 0.01] and LAWT(SD) [0.68 (0.61-0.71) vs. 0.60 (0.56-0.65); p < 0.001] were significantly greater in AF alone vs. HFpEF alone even after multi-variate adjustment and propensity matching. After excluding the HFpEF+AF group, both LAWV and LAWT [SD] provided incremental values when added to PALS or LAVi (all p for net reclassification improvement <0.05) in discriminating AF alone, with LAWT[SD] yielding the largest C-statistic (0.78, 95% CI: 0.70-0.86) among all LA wall indices.
Conclusions: Despite a similar extent of LA enlargement and dysfunction in HFpEF vs. AF alone, larger LAWV and LAWT [SD] can distinguish AF from HFpEF alone, suggesting the distinct underlying pathophysiological mechanism of LA remodeling in AF vs. HFpEF.
Keywords: atrial fibrillation; heart failure with preserved ejection fraction; left atrial remodeling; left atrial wall; multi-detector computed tomography; strain.
Copyright © 2022 Kuo, Jin, Sun, Chang, Chi, Sung, Mok, Yun, Chang, Chung, Yu, Wu, Hung, Yeh and Lam.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources