

The clinical features, management, and survival of elderly patients with gastric cancer
- PMID: 35557576
- PMCID: PMC9086038
- DOI: 10.21037/jgo-22-280
The clinical features, management, and survival of elderly patients with gastric cancer
Abstract
Background: It is anticipated that the number of elderly patients with gastric cancer (GC) will increase with population aging; however, most studies on GC set the upper age limit at 80 years old, studies on the prognosis of elderly patients with GC over 80 years old is very limited. In this study, we conducted a retrospective analysis of this sub-cohort.
Methods: This retrospective cohort study aimed to analyze the clinical data of patients aged >80 who died of GC in People's Liberation Army General Hospital between 1985 and 2020. We collected clinical informations about pathological GC types, differentiation degrees, clinical stages, anatomic sites and Bormann types of the selected case. Characteristics of participants, such as smoking, drinking, and tumor history, age, gender, and complications, were also recorded. The Kaplan-Meier method, a multivariate Cox multivariate proportional hazard model, and logistic regression were used to analyze the patient overall survival (OS) rates and treatment outcomes.
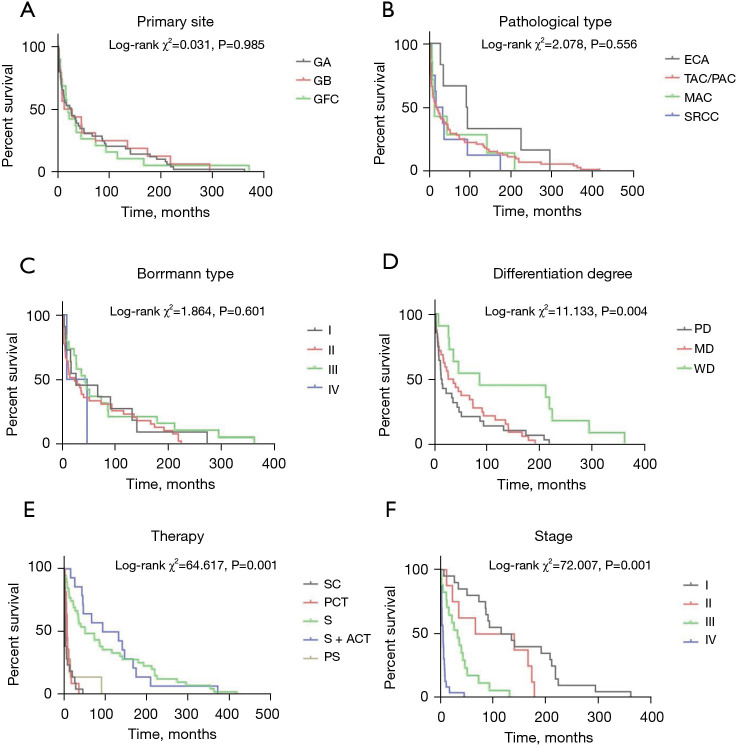
Results: The study included 92 patients (83.7% men) with a median OS of 45 months. The most common site for GC was the gastric antrum (GA), the most common site of metastatic spread was the liver, and the most common pathological GC type was tubular adenocarcinoma/papillary adenocarcinoma (TAC/PAC). Furthermore, the prevalent complications were hypertension, coronary heart disease, and diabetes. Diabetes was a risk factor affecting the total survival time [hazard ratio (HR) =2.326, P=0.029]. The most often-used GC treatment was curative surgery. The survival time was significantly longer in the curative surgery group and curative surgery + adjuvant chemotherapy group compared with the support care group (HR =0.119, P=0.001; HR =0.110, P=0.001). There was no significant difference in survival time among the palliative chemotherapy group, palliative surgery group, and support care group. Tumor staging was significantly correlated with OS rate, the median survival time of patients at stage III and stage IV GC were significantly lower than the median survival time of patients at stage I GC (HR =6.235, P=0.001; HR =30.955, P=0.001).
Conclusions: For patients over 80 years old with good physical conditions in the early stage of GC, more active treatment can still bring better prognosis.
Keywords: Gastric cancer (GC); elderly; patient; survival analysis; therapy.
2022 Journal of Gastrointestinal Oncology. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jgo.amegroups.com/article/view/10.21037/jgo-22-280/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Association of Tumor-Associated Collagen Signature With Prognosis and Adjuvant Chemotherapy Benefits in Patients With Gastric Cancer.JAMA Netw Open. 2021 Nov 1;4(11):e2136388. doi: 10.1001/jamanetworkopen.2021.36388. JAMA Netw Open. 2021. PMID: 34846524 Free PMC article.
-
[Safety and efficacy of adjuvant chemotherapy with oxaliplatin and S-1 for patients with locally advanced gastric cancer after D2 lymph nodes dissection].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Feb 25;24(2):145-152. doi: 10.3760/cma.j.cn.441530-20201016-00561. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 33508920 Chinese.
-
[A multi-center retrospective study of perioperative chemotherapy for gastric cancer based on real-world data].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 May 25;24(5):403-412. doi: 10.3760/cma.j.cn.441530-20200111-00014. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 34000769 Chinese.
-
Canine Gastric Cancer: Current Treatment Approaches.Vet Sci. 2022 Jul 26;9(8):383. doi: 10.3390/vetsci9080383. Vet Sci. 2022. PMID: 35893776 Free PMC article. Review.
-
Current practice for gastric cancer treatment in Ukraine.Transl Gastroenterol Hepatol. 2017 May 16;2:47. doi: 10.21037/tgh.2017.04.07. eCollection 2017. Transl Gastroenterol Hepatol. 2017. PMID: 28616603 Free PMC article. Review.
Cited by
-
Systematic review and meta-analysis of reports of patients with gastric cancer aged 80 years and older.Int Cancer Conf J. 2022 Jul 6;11(4):224-230. doi: 10.1007/s13691-022-00563-w. eCollection 2022 Oct. Int Cancer Conf J. 2022. PMID: 36186225 Free PMC article. Review.
References
-
- Global Burden of Disease Cancer Collaboration ; Fitzmaurice C, Abate D, et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol 2019;5:1749-68. 10.1001/jamaoncol.2019.2996 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous