

Oxygenation Performance of Different Non-Invasive Devices for Treatment of Decompression Illness and Carbon Monoxide Poisoning
- PMID: 35557974
- PMCID: PMC9090223
- DOI: 10.3389/fphys.2022.885898
Oxygenation Performance of Different Non-Invasive Devices for Treatment of Decompression Illness and Carbon Monoxide Poisoning
Abstract
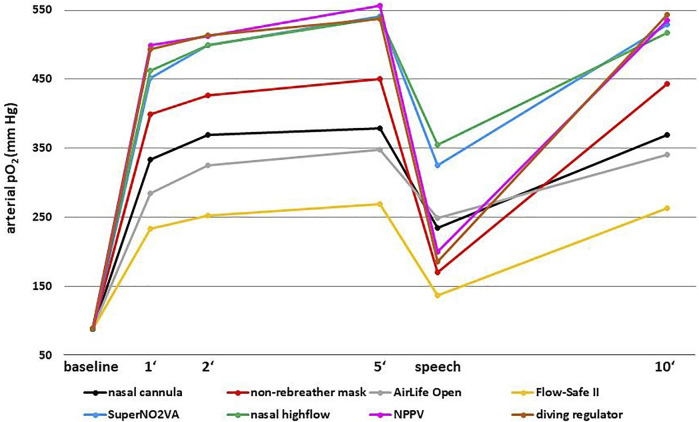
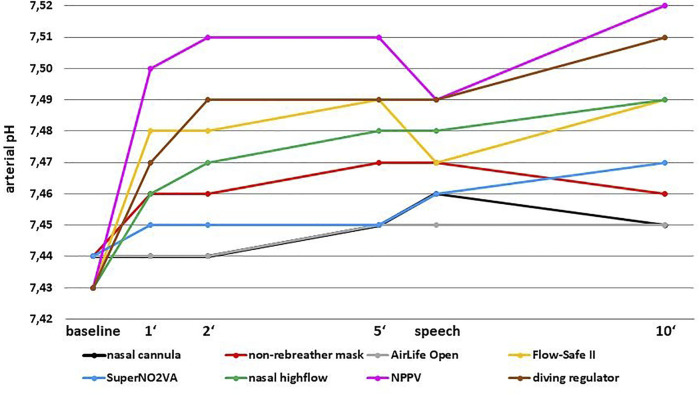
Study Objective: Application of high concentrations of oxygen to increase oxygen partial pressure (pO2) is the most important treatment for patients with carbon monoxide intoxication or divers with suspected decompression illness. The aim of this study was to evaluate the oxygenation performance of various non-invasive oxygen systems. Methods: The effect of different oxygen systems on arterial pO2, pCO2 and pH and their subjective comfort was evaluated in 30 healthy participants. Eight devices were included: nasal cannula, non-rebreather mask, AirLife Open mask, Flow-Safe II CPAP device, SuperNO2VA nasal PAP device, all operated with 15 L/min constant flow oxygen; nasal high-flow (50 L/min flow, 1.0 FiO2), non-invasive positive pressure ventilation (NPPV, 12 PEEP, 4 ASB, 1.0 FiO2) and a standard diving regulator (operated with pure oxygen). Results: Diving regulator, SuperNO2VA, nasal high-flow and NPPV achieved mean arterial pO2 concentrations between 538 and 556 mm Hg within 5 minutes. The AirLife Open mask, the nasal cannula and the non-rebreather mask achieved concentrations of 348-451 mm Hg and the Flow-Safe II device 270 mm Hg. Except for the AirLife open mask, pCO2 decreased and pH increased with all devices. The highest pH values were observed with NPPV, diving regulator, Flow-Safe II and nasal high-flow but apparent hyperventilation was uncommon. The AirLife Open and the non-rebreather mask were the most comfortable, the SuperNO2VA and the nasal cannula the most uncomfortable devices. Conclusion: A standard diving regulator and the SuperNO2VA device were equally effective in providing highest physiologically possible pO2 as compared to nasal high-flow and NPPV.
Keywords: PaO2; arterial oxygen partial pressure; carbon monoxide poisoning; decompression illness; diving accident; non-invasive ventilation; oxygen masks.
Copyright © 2022 Köhler, Zoll, Ploner, Hammer, Joannidis, Tilg, Finkenstedt and Hartig.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Comparison of a simplified nasal continuous positive airways pressure device with nasal cannula in obese patients undergoing colonoscopy during deep sedation: A randomised clinical trial.Eur J Anaesthesiol. 2019 Sep;36(9):633-640. doi: 10.1097/EJA.0000000000001052. Eur J Anaesthesiol. 2019. PMID: 31313720 Clinical Trial.
-
Best clinical practices for the sleep center adjustment of noninvasive positive pressure ventilation (NPPV) in stable chronic alveolar hypoventilation syndromes.J Clin Sleep Med. 2010 Oct 15;6(5):491-509. J Clin Sleep Med. 2010. PMID: 20957853 Free PMC article.
-
Comparison of tissue oxygenation achieved breathing oxygen using different delivery devices and flow rates.Diving Hyperb Med. 2020 Mar 31;50(1):34-42. doi: 10.28920/dhm50.1.34-42. Diving Hyperb Med. 2020. PMID: 32187616 Free PMC article.
-
Treatment of carbon monoxide poisoning: high-flow nasal cannula versus non-rebreather face mask.Clin Toxicol (Phila). 2021 May;59(5):386-391. doi: 10.1080/15563650.2020.1817477. Epub 2020 Sep 22. Clin Toxicol (Phila). 2021. PMID: 32959716
-
Effect of high-flow nasal cannula oxygen therapy in patients with chronic obstructive pulmonary disease: A meta-analysis.J Clin Nurs. 2022 Jan;31(1-2):87-98. doi: 10.1111/jocn.15957. Epub 2021 Jul 9. J Clin Nurs. 2022. PMID: 34245049 Review.
Cited by
-
Carbon Monoxide Poisoning: Diagnosis, Prognostic Factors, Treatment Strategies, and Future Perspectives.Diagnostics (Basel). 2025 Feb 27;15(5):581. doi: 10.3390/diagnostics15050581. Diagnostics (Basel). 2025. PMID: 40075828 Free PMC article. Review.
-
S2k guideline for diving accidents.Ger Med Sci. 2023 Mar 3;21:Doc01. doi: 10.3205/000315. eCollection 2023. Ger Med Sci. 2023. PMID: 37033772 Free PMC article.
-
Physiological monitoring to prevent diving disorders.Front Physiol. 2024 Dec 18;15:1517361. doi: 10.3389/fphys.2024.1517361. eCollection 2024. Front Physiol. 2024. PMID: 39744705 Free PMC article. Review.
-
Effect of a helium and oxygen mixture on physiological parameters of rats with cerebral arterial air embolism.Front Physiol. 2024 May 13;15:1388331. doi: 10.3389/fphys.2024.1388331. eCollection 2024. Front Physiol. 2024. PMID: 38803366 Free PMC article.
References
-
- Brubakk A., Neumann T. (2002). Bennett and Elliotts' Physiology and Medicine of Diving. 5th edition, 9780702025716. Saunders Limited.
LinkOut - more resources
Full Text Sources
Research Materials