

Risk Factors and Biomarkers for Immune-Related Adverse Events: A Practical Guide to Identifying High-Risk Patients and Rechallenging Immune Checkpoint Inhibitors
- PMID: 35558065
- PMCID: PMC9086893
- DOI: 10.3389/fimmu.2022.779691
Risk Factors and Biomarkers for Immune-Related Adverse Events: A Practical Guide to Identifying High-Risk Patients and Rechallenging Immune Checkpoint Inhibitors
Abstract
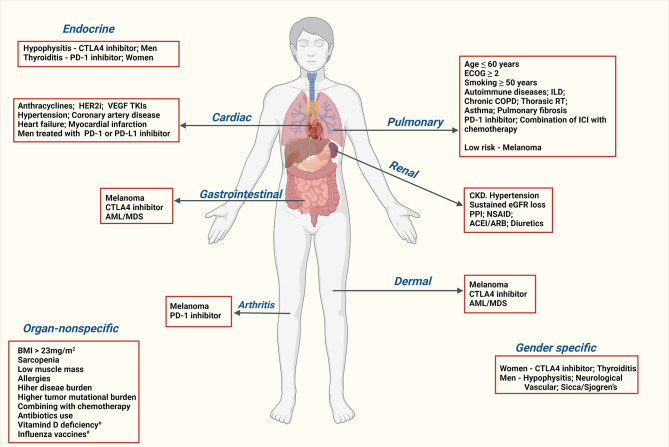
Immune-related adverse events (irAEs) are a range of complications associated with the use of immune-checkpoint inhibitors (ICIs). Two major classes of ICIs widely used are Cytotoxic T-Lymphocyte Antigen 4 (CTLA4) and Programmed Cell death-1 (PD-1)/Programmed death-ligand 1 (PD-L1) inhibitors. High-grade irAEs are life-threatening and often cause a severe decline in performance status in such that patients do not qualify for any further anticancer treatments. It is difficult to generalize the evidence in the current literature on risk factors or biomarkers for the entire class of ICIs as the studies so far are either disease-specific (e.g., lung cancer or melanoma) or ICI agent-specific (e.g., pembrolizumab, ipilimumab) or irAE-specific (e.g., pneumonitis or gastritis). In this review, risk factors and biomarkers to consider before initiating or monitoring ICI are listed with a practical purpose in day-to-day practice. Risk factors are grouped into demographics and social history, medical history, and medication history, tumor-specific and agent-specific risk factors. A higher risk of irAE is associated with age <60 years, high body mass index, women on CTLA4 and men on PD-1/PD-L1 agents, and chronic smokers. Patients with significant kidney (Stage IV-V), cardiac (heart failure, coronary artery disease, myocardial infarction, hypertension), and lung (asthma, pulmonary fibrosis, and chronic obstructive pulmonary disease) are at a higher risk of respective organ-specific irAEs. Pre-existing autoimmune disease and chronic use of certain drugs (proton pump inhibitors, diuretics, anti-inflammatory drugs) also increase the irAE-risk. Biomarkers are categorized into circulating blood counts, cytokines, autoantibodies, HLA genotypes, microRNA, gene expression profiling, and serum proteins. The blood counts and certain protein markers (albumin and thyroid-stimulating hormone) are readily accessible in current practice. High neutrophil-lymphocyte ratio, eosinophil/monocyte/lymphocyte counts; TSH and troponins at diagnosis and drop in the white count and lymphocyte count can predict irAE. Other biomarkers with limited evidence are cytokines, autoantibodies, HLA genotypes, microRNA, and gene expression profiling. With fast-expanding approvals for ICIs in various cancer types, knowledge on risk factors and biomarkers can help providers assess the irAE-risk of their patients. Prospective disease and agent-specific studies are needed to provide further insight on this essential aspect of ICI therapy.
Keywords: biomarkers; colitis; immune checkpoint inhibitors; immune related adverse events; pneumonitis; predictors; rechallenge; risk factors.
Copyright © 2022 Chennamadhavuni, Abushahin, Jin, Presley and Manne.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Ascierto PA, Bono P, Bhatia S, Melero I, Nyakas MS, Svane IM, et al. LBA18 - Efficacy of BMS-986016, a Monoclonal Antibody That Targets Lymphocyte Activation Gene-3 (LAG-3), in Combination With Nivolumab in Pts With Melanoma Who Progressed During Prior Anti–PD-1/PD-L1 Therapy (Mel Prior IO) in All-Comer and Biomarker-Enriched Populations. Ann Oncol (2017) 28:v611–2. doi: 10.1093/annonc/mdx440.011 - DOI
-
- Siu LL, Steeghs N, Meniawy T, Joerger M, Spratlin JL, Rottey S, et al. Preliminary Results of a Phase I/IIa Study of BMS-986156 (Glucocorticoid-Induced Tumor Necrosis Factor Receptor–Related Gene [GITR] Agonist), Alone and in Combination With Nivolumab in Pts With Advanced Solid Tumors. J Clin Oncol (2017) 35(15_suppl):104–4. doi: 10.1200/JCO.2017.35.15_suppl.104 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials