

Development of a Novel Immune-Related Gene Prognostic Index for Breast Cancer
- PMID: 35558081
- PMCID: PMC9086776
- DOI: 10.3389/fimmu.2022.845093
Development of a Novel Immune-Related Gene Prognostic Index for Breast Cancer
Abstract
Objective: To construct an immune-related gene prognostic index (IRGPI) for breast cancer (BC) and investigate its prognostic specificity and the molecular and immune characteristics.
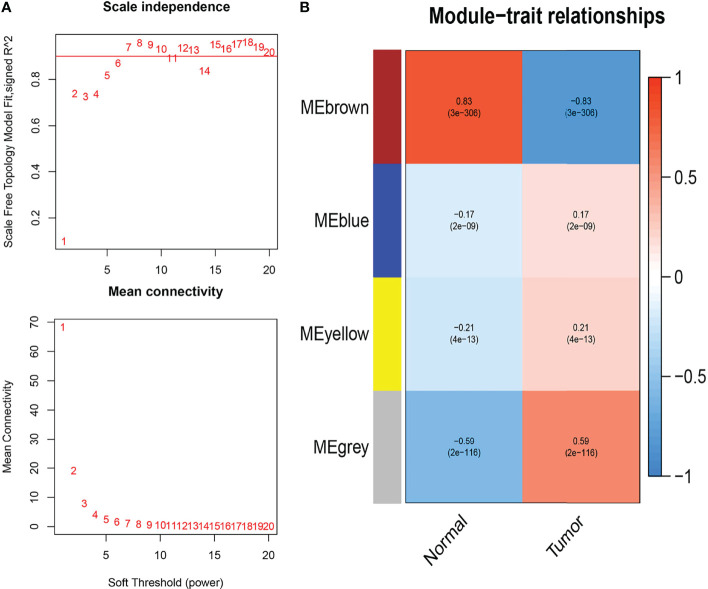
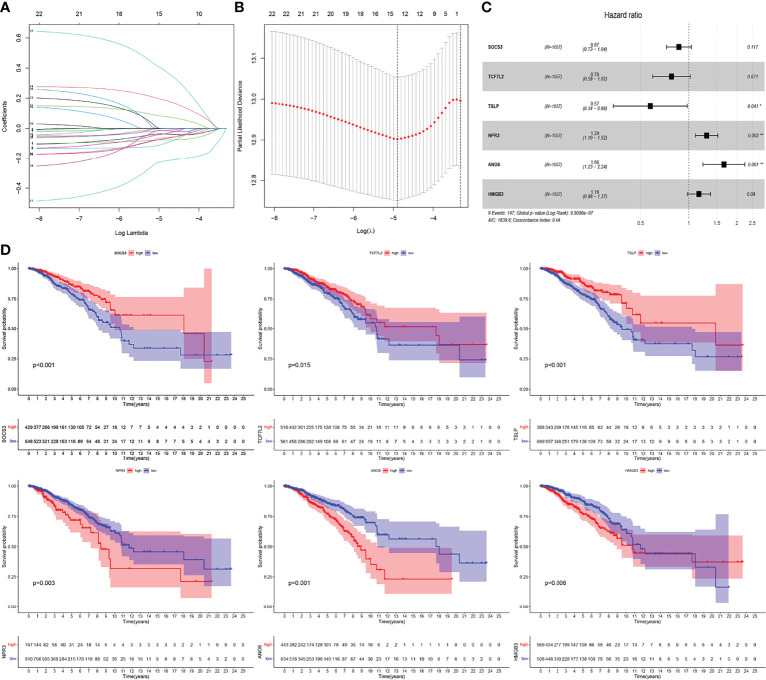
Methods: BC hub genes were identified from The Cancer Genome Atlas and immune-related databases using weighted gene co-expression network analysis (WGCNA). IRGPI was constructed using univariate, LASSO, and multivariate regression analyses, and was validated with GSE58812 and GSE97342 in the Gene Expression Omnibus database (GEO). At the same time, we evaluated the predictive ability of IRGPI for different BC subtypes. Subsequently, the molecular and immune characteristics, clinical relevance, and benefits of immune checkpoint inhibitor treatment were analyzed for different IRGPI subgroups.
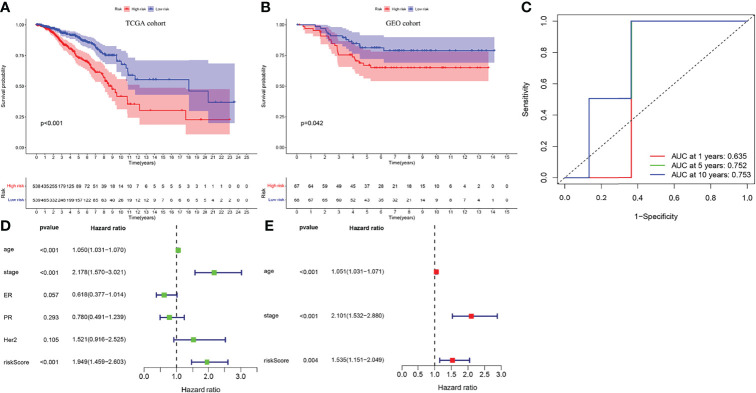
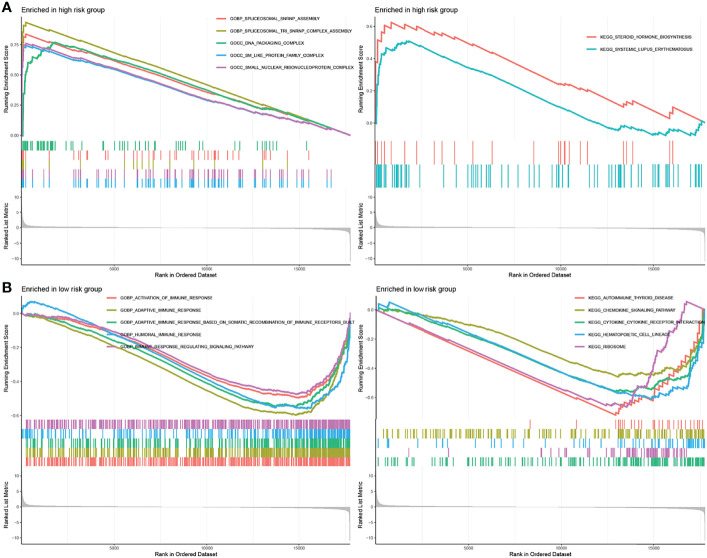
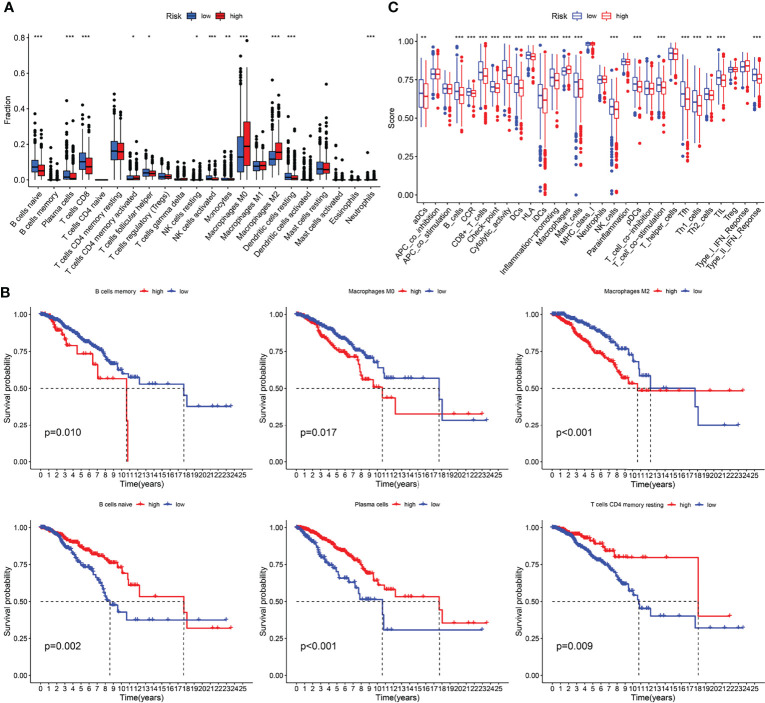
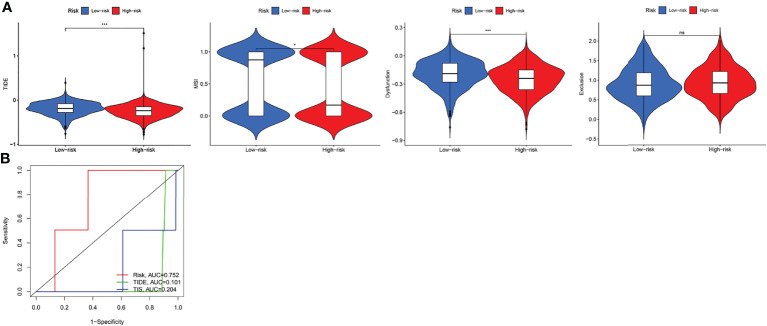
Results: IRGPI consisted of six genes: SOCS3, TCF7L2, TSLP NPR3, ANO6, and HMGB3. The IRGPI 1-, 5-, and 10-years area under curve (AUC) values were 0.635, 0.752, and 0.753, respectively, indicating that IRGPI has good potential in predicting the long-term survival of BC patients, consistent with the results in the GEO cohort. IRGPI showed good predictive power in four different breast cancer subtypes: ER positive, PR positive, HER2 positive and triple-negative (P<0.01). Compared with the low-IRGPI group, the high-IRGPI group had a worse prognosis and a lower degree of immune infiltrating cells (p < 0.05). IRGPI showed specificity in distinguishing age, TNM stage, ER, and HER2 statuses, and our study found that the high-IRGPI group had low tumor immune dysfunction and exclusion (TIDE), microsatellite instability (MSI), and T cell dysfunction scores (p < 0.05). In addition, compared with the TIDE and TIS models, showed that the AUCs of IRGPI were better during the 5-year follow-up.
Conclusion: IRGPI can be used as an independent prognostic indicator of breast cancer, providing a method for monitoring the long-term treatment of BC.
Keywords: WGCNA; breast cancer; immune checkpoint inhibitor; immune-related genes; prognostic index.
Copyright © 2022 Yao, Kong, Liu, Xu, Liu and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Fitzmaurice C, Abate D, Abbasi N, Abbastabar H, Abd-Allah F, Abdel-Rahman O, et al. . Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol (2019) 5(12):1749–68. doi: 10.1001/jamaoncol.2019.2996 - DOI - PMC - PubMed
-
- Salerno E, Culakova E, Kleckner A, Heckler C, Lin P, Matthews C, et al. . Physical Activity Patterns and Relationships With Cognitive Function in Patients With Breast Cancer Before, During, and After Chemotherapy in a Prospective, Nationwide Study. J Clin Oncol Off J Am Soc Clin Oncol (2021) 39 (29):3283–92. doi: 10.1200/jco.20.03514 - DOI - PMC - PubMed
-
- Moy B, Rumble R, Come S, Davidson N, Di Leo A, Gralow J, et al. . Chemotherapy and Targeted Therapy for Patients With Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer That is Either Endocrine-Pretreated or Hormone Receptor-Negative: ASCO Guideline Update. J Clin Oncol Off J Am Soc Clin Oncol (2021) 39(35):3938–58 JCO2101374. doi: 10.1200/jco.21.01374 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous