

A Multicenter Analysis of Changes in Pediatric Antibiotic Susceptibilities Among Staphylococcus aureus and Pseudomonas aeruginosa Isolates: 2014-2018
- PMID: 35558344
- PMCID: PMC9088438
- DOI: 10.5863/1551-6776-27.4.330
A Multicenter Analysis of Changes in Pediatric Antibiotic Susceptibilities Among Staphylococcus aureus and Pseudomonas aeruginosa Isolates: 2014-2018
Abstract
Objective: To describe antibiotic susceptibilities for Staphylococcus aureus and Pseudomonas aeruginosa among pediatric institutions in 2018. To assess correlations between antibiotic utilization and susceptibilities.
Methods: Institutional antibiograms from 2018 were compiled among 13 institutions via a survey. Resistant pathogens and antibiotic days of therapy/1000 patient days (PD) were collected from 6 institutions over 5 years. Correlations were assessed as pooled data among all institutions and relative changes within individual institutions.
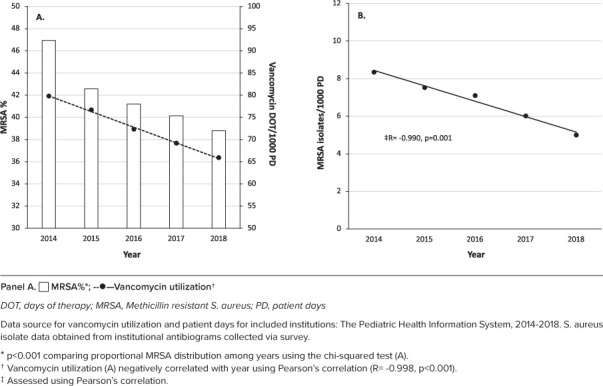
Results: All 8552 S aureus isolates in 2018 were vancomycin susceptible and 40.1% were methicillin resistant (MRSA). Among MRSA, 96.3% and 78.8% were susceptible to trimethoprim/sulfamethoxazole and clindamycin, respectively. Pooled yearly MRSA/1000 PD decreased from 2014-2018 and correlated with pooled yearly decreases in vancomycin utilization (R = 0.983, p = 0.003). Institutional relative decreases in vancomycin utilization from 2014-2018 did not correlate with institutional relative decreases in MRSA susceptibility (R = -0.659, p = 0.16). Susceptibility to meropenem was 90.9% among 2315 P aeruginosa isolates in 2018. Antipseudomonal beta-lactam susceptibility ranged from 89.4% to 92.3%. Pooled yearly meropenem-resistant P aeruginosa/1000 PD and meropenem utilization did not significantly decrease over time or correlate (both p > 0.6). Institutional relative change in meropenem utilization from 2013-2017 correlated with the institutional relative change in P aeruginosa susceptibility to meropenem from 2014-2018 (Rs = -0.89, p = 0.019).
Conclusions: Among included institutions, the burden of MRSA decreased over time. Institutional MRSA prevalence did not consistently correlate with institutional vancomycin utilization. Institutional changes in meropenem utilization correlated with P aeruginosa susceptibility the following year. Pooled analyses did not illustrate this correlation, likely owing to variability in utilization between institutions.
Keywords: Pseudomonas aeruginosa; Staphylococcus aureus; antibiotic resistance; antimicrobial stewardship; meropenem; pediatrics; vancomycin.
Copyright. Pediatric Pharmacy Association. All rights reserved. For permissions, email: mhelms@pediatricpharmacy.org 2022.
Conflict of interest statement
Disclosures. Three authors (JSS, EB, FB) are members of the PPA PBRN. Otherwise, the authors declare no conflicts or financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, and honoraria. JSS and KRL had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Figures



References
-
- Larru B, Gong W, Vendetti N et al. Bloodstream infections in hospitalized children: epidemiology and antimicrobial susceptibilities. Pediatr Infect Dis J . 2016;35(5):507–510. - PubMed
-
- Hamdy RF, Dona D, Jacobs MB, Gerber JS. Risk factors for complications in children with Staphylococcus aureus bacteremia. J Pediatr . 2019;208:214–220.e2. - PubMed
LinkOut - more resources
Full Text Sources