

Prognostic Factors and Survival Benefits of Antitumor Treatments for Advanced Non-Small Cell Lung Cancer Patients With Central Nervous System Metastasis With or Without Driver Genes: A Chinese Single-Center Cohort Study
- PMID: 35558520
- PMCID: PMC9090435
- DOI: 10.3389/fonc.2022.879554
Prognostic Factors and Survival Benefits of Antitumor Treatments for Advanced Non-Small Cell Lung Cancer Patients With Central Nervous System Metastasis With or Without Driver Genes: A Chinese Single-Center Cohort Study
Abstract
Background: The prognosis of non-small cell lung cancer (NSCLC) patients with central nervous system (CNS) metastasis is poor. The treatment for CNS metastasis could prolong the overall survival of NSCLC patients. We aimed to investigate the prognostic factors of Chinese NSCLC patients with CNS metastasis and the survival benefits of various treatments for CNS metastasis in NSCLC patients with or without driver genes.
Methods: Based on the CAPTRA-Lung database, NSCLC patients with CNS metastasis admitted at the Peking Union Medical College Hospital between January 2010 and October 2018 were enrolled in the study. The prognostic factors were analyzed using univariate and multivariate Cox regression analyses.
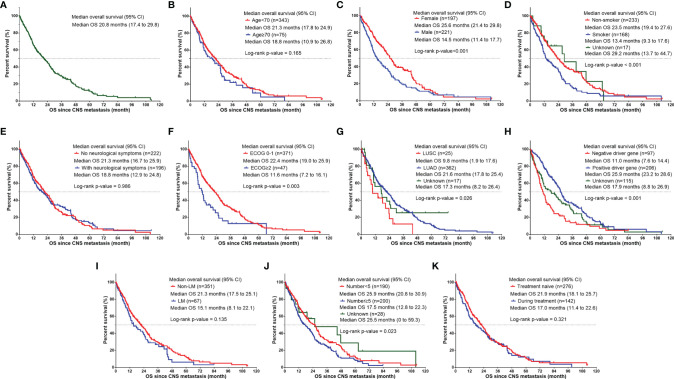
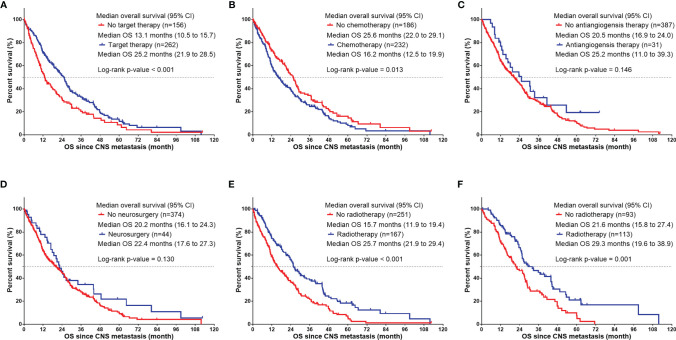
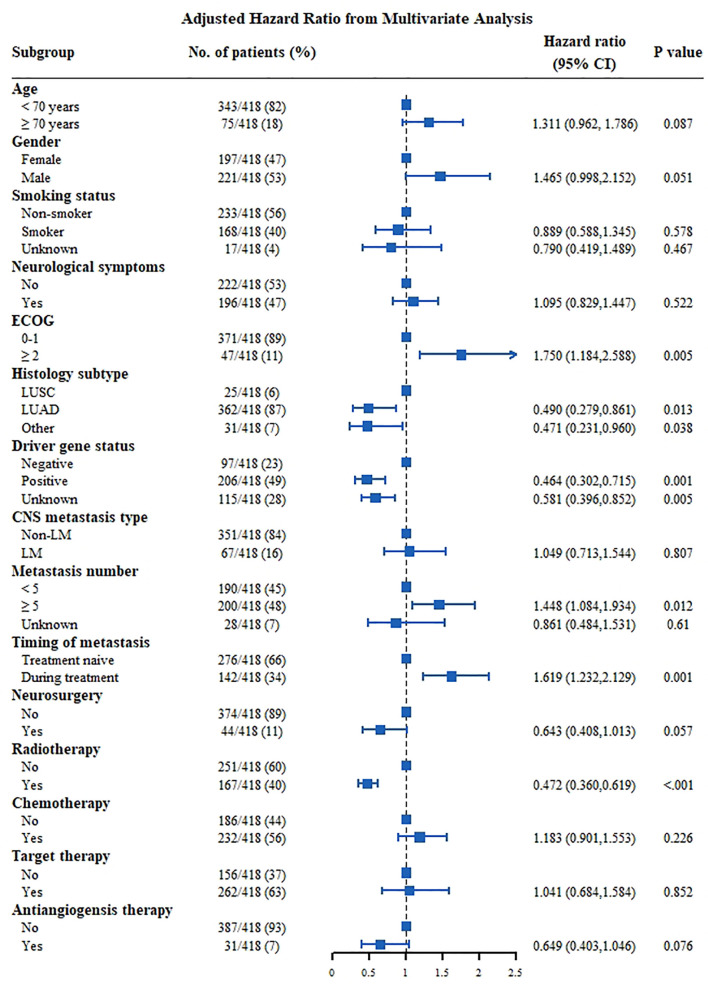
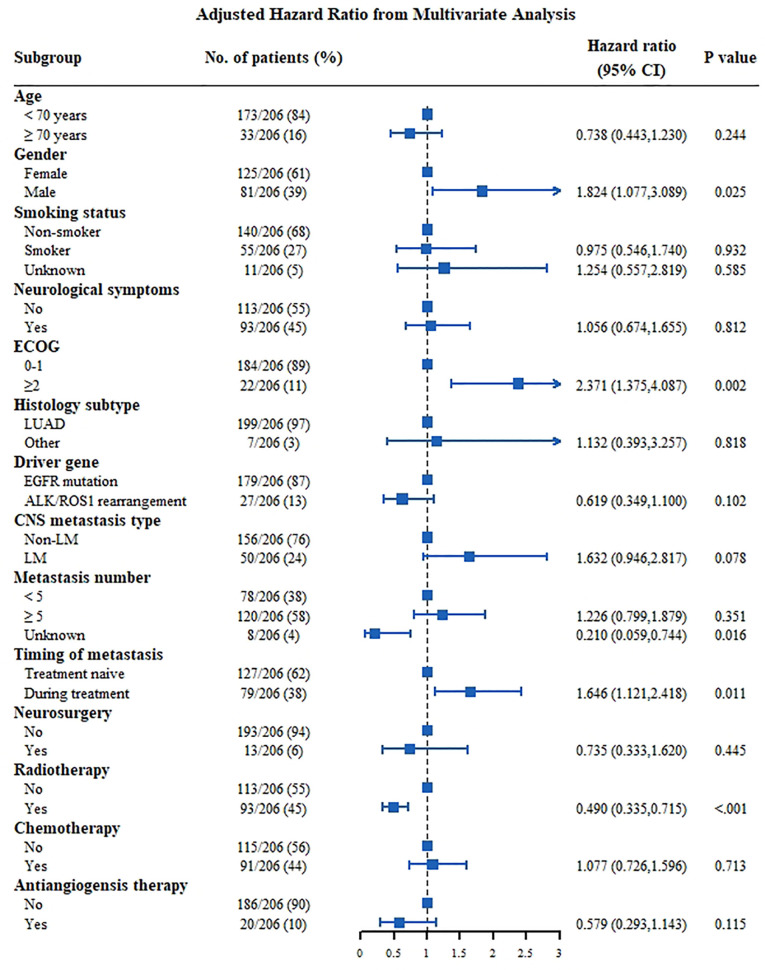
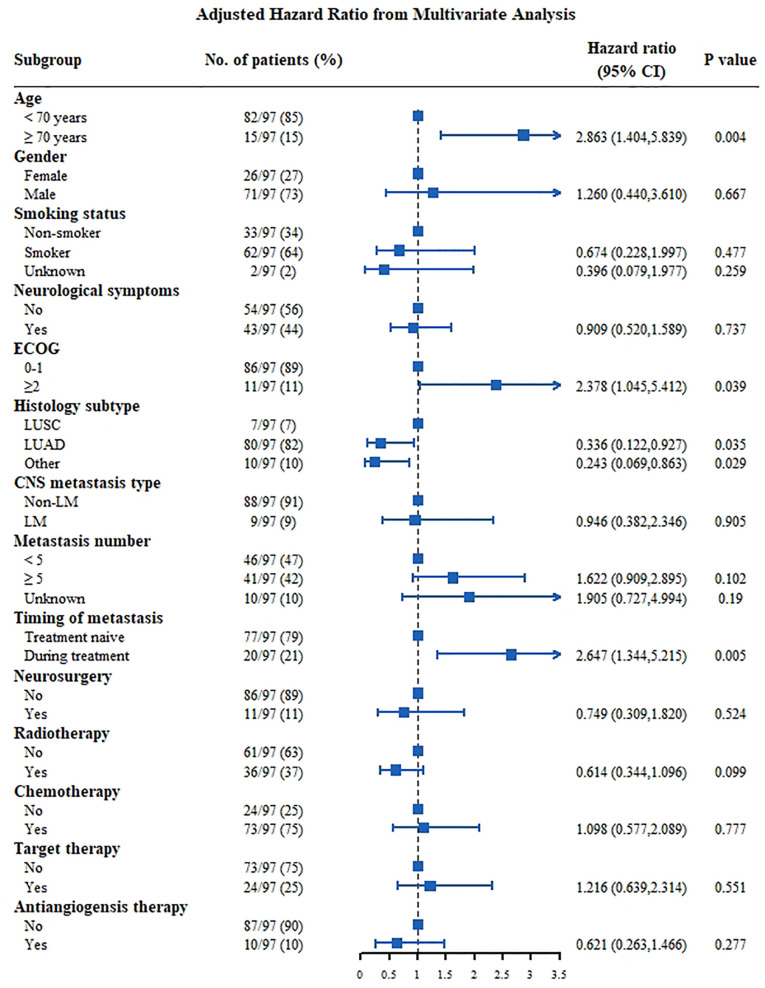
Results: Overall, 418 patients were enrolled in the study. A total of 206 patients (49.3%) had CNS metastasis with positive driver genes, while 97 patients (23.2%) had negative driver genes. The median survival time after CNS metastasis was 20.8 months. In the multivariable analysis, an Eastern Cooperative Oncology Group performance status of ≥2 (hazard ratio [HR]: 1.750, 95% confidence interval [CI]: 1.184-2.588, P=0.005), number of CNS metastases ≥5 (HR: 1.448, 95% CI: 1.084 -1.934, P=0.012), and CNS metastasis developed during treatment (HR: 1.619, 95% CI: 1.232-2.129, P=0.001) were independent risk factors for poor survival. Lung adenocarcinoma (HR: 0.490, 95% CI: 0.279-0.861, P=0.013) and driver gene positivity (HR: 0.464, 95% CI: 0.302-0.715, P=0.001) were independent predictors of prolonged survival. Radiotherapy for CNS metastasis showed a survival benefit in NSCLC patients in the entire groups (HR: 0.472, 95% CI: 0.360-0.619, P <0.001), and in patients with positive driver genes.
Conclusion: Performance status, number of CNS metastases, timing of CNS metastasis, histological subtype, and driver gene status are prognostic factors for NSCLC patients with CNS metastasis. Furthermore, radiotherapy improved the survival in NSCLC patients with CNS metastasis.
Keywords: central nervous system metastasis; cohort study; non-small-cell lung cancer; prognostic factors; treatment outcome.
Copyright © 2022 Gao, Chen, Liu, Shi, Liang, Zhou, Zhao, Pan, Zhong, Xu and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources