

Risk Factors and Medical Resource Utilization of Respiratory Syncytial Virus, Human Metapneumovirus, and Influenza-Related Hospitalizations in Adults-A Global Study During the 2017-2019 Epidemic Seasons (Hospitalized Acute Respiratory Tract Infection [HARTI] Study)
- PMID: 35559130
- PMCID: PMC9088513
- DOI: 10.1093/ofid/ofab491
Risk Factors and Medical Resource Utilization of Respiratory Syncytial Virus, Human Metapneumovirus, and Influenza-Related Hospitalizations in Adults-A Global Study During the 2017-2019 Epidemic Seasons (Hospitalized Acute Respiratory Tract Infection [HARTI] Study)
Abstract
Background: Respiratory syncytial virus (RSV), human metapneumovirus (hMPV), and influenza are respiratory pathogens leading to hospitalization in adults. Our understanding of the disease burden is limited to data from single-center or 1-season studies in elderly patients. The HARTI study allows comparison of risk factors for progression to severe disease and medical resources utilization (MRU) during and post-hospitalization in adults diagnosed with influenza, RSV, or hMPV.
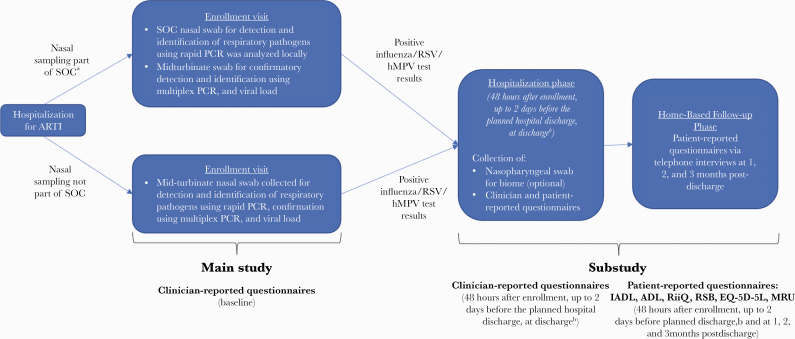
Methods: This was a prospective global study in adults hospitalized with acute respiratory tract infection (40 centers, 12 countries). Participants with influenza, RSV, or hMPV were enrolled in a substudy and followed for up to 3 months postdischarge.
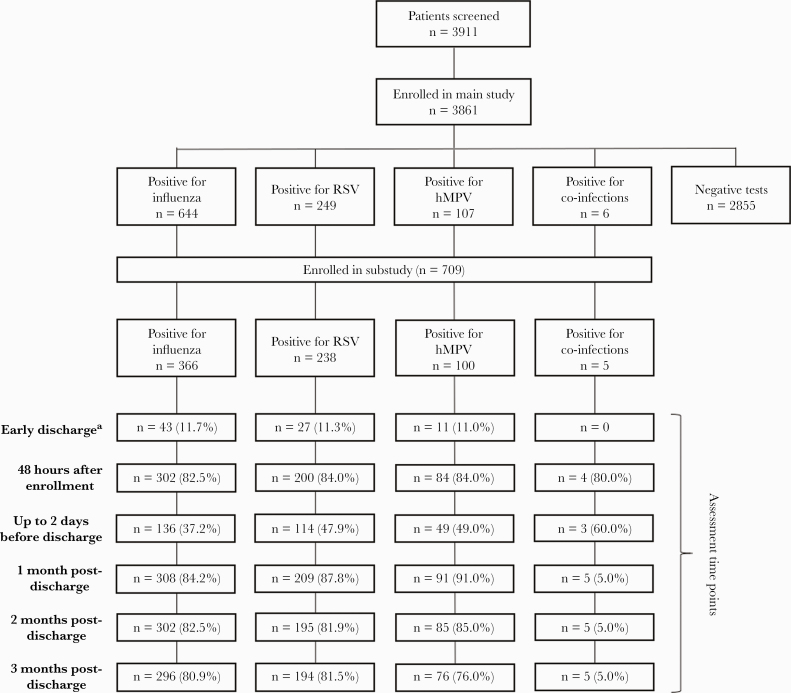
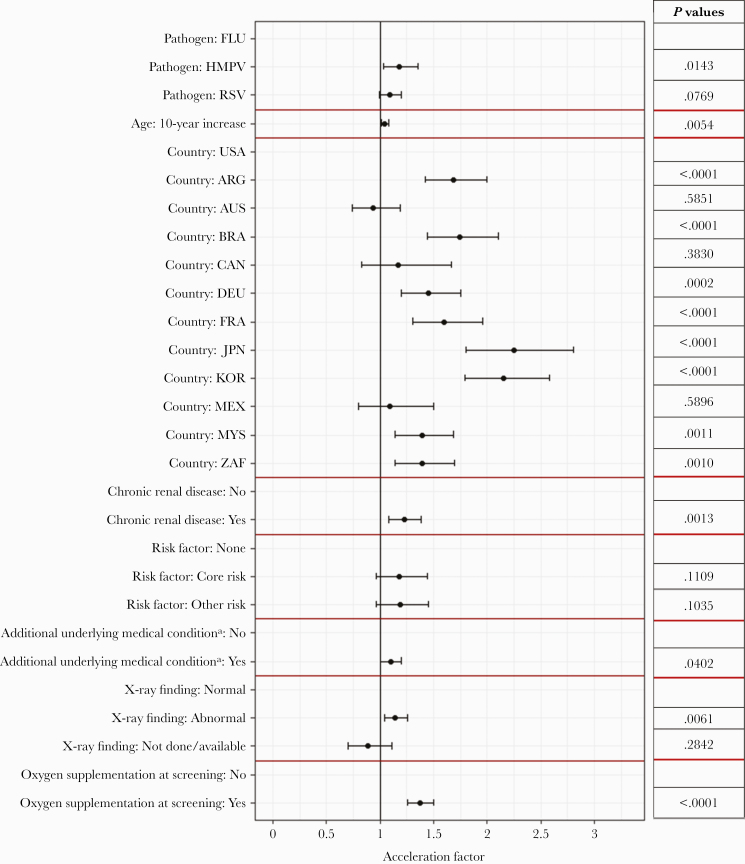
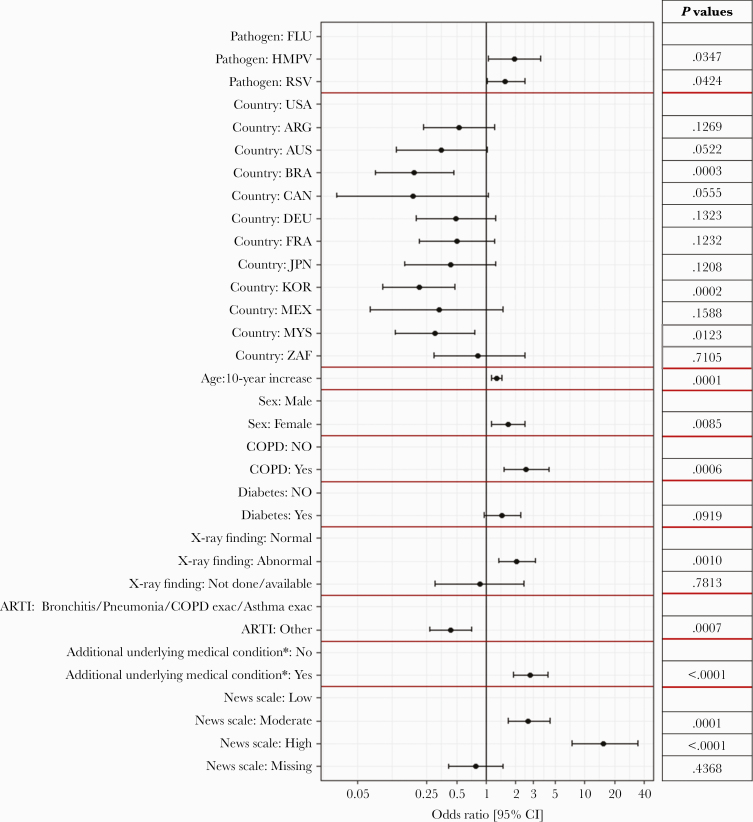
Results: Overall, 366 influenza, 238 RSV, and 100 hMPV-infected participants enrolled in the substudy. RSV participants were older and had greater frequency of risk factors and longer duration of symptoms before hospitalization than influenza participants. The RSV and hMPV groups received more bronchodilators, corticosteroids, and oxygen supplementation. No significant differences in intensive care unit admissions or complications were observed. Readmission occurred in 20%-33% of patients within 3 months postdischarge, with the highest rates for RSV and hMPV. In-hospital death occurred in 2.5% of RSV, 1.6% of influenza, and 2% of hMPV participants. In multivariate analyses, length of stay was independently associated with country, renal disease, and increased age; probability of receiving supplemental oxygen was associated with pathogen (hMPV > RSV > influenza), abnormal chest x-ray, and increased age.
Conclusions: Although influenza is more frequent, the HARTI study demonstrates greater frequency of underlying risk factors and MRU for RSV and hMPV vs influenza in hospitalized adults, indicating a need for effective interventions.
Keywords: Influenza; RSV; global prospective study; hMPV; medical resource utilization.
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Troeger C, Forouzanfar M, Rao PC, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis 2016; 18:1191–210. - PMC - PubMed
-
- Nicholson KG, Webster RG, Hay A.. Textbook of Influenza. Blackwell Science Ltd; 1998.
