

doi: 10.1182/blood.2021014588.
Monoclonal and oligoclonal anti-platelet factor 4 antibodies mediate VITT
Affiliations
- PMID: 35560046
- PMCID: PMC9262283
- DOI: 10.1182/blood.2021014588
Item in Clipboard
Monoclonal and oligoclonal anti-platelet factor 4 antibodies mediate VITT
Blood.
.
Abstract
Kanack and colleagues analyze anti-platelet factor 4 antibodies from 5 patients with vaccine-induced thrombotic thrombocytopenia (VITT) secondary to COVID-19 adenoviral vaccination and antibodies from patients with spontaneous heparin-induced thrombocytopenia (HIT) and classical HIT. VITT antibodies are monoclonal or oligoclonal, similar to spontaneous HIT, whereas classical HIT antibodies are polyclonal. Heparin inhibits antibody-induced platelet activation in VITT, suggesting that heparin should be considered for the treatment of VITT.
Figures
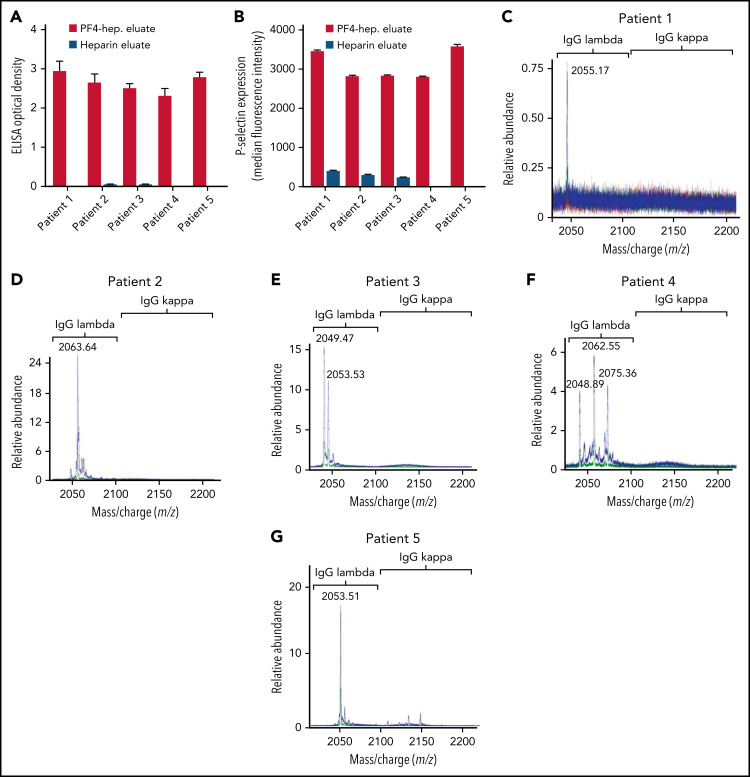
VITT antibodies are monoclonal or oligoclonal. (A-B) Eluates from PF4-heparin beads and control heparin beads were evaluated in PF4-polyanion ELISA for binding to PF4-polyvinylsulfonate complexes and for platelet activation in the PEA. Means and SD (n = 3) are shown. Control (heparin) bead studies were not performed with patients 4 and 5 because of limited sample volume. (C-G) Displayed are LC-ESI-QTOF MS light chain +11 (mass to charge [m/z]) distributions from anti-PF4 antibodies isolated from 5 patients with VITT. In the spectra, green represents the distribution of all λ-containing Ig’s, red represents the +11 m/z distribution of all κ-containing Ig’s, and blue represents the +11 m/z light chain distribution of κ and λ light chains associated with an IgG heavy chain. The number listed above the peaks indicates the +11 m/z ratio of the identified light chain. The x-axis shows m/z ratios, and the y-axis shows the relative abundance of the monoclonal or oligoclonal antibody identified.
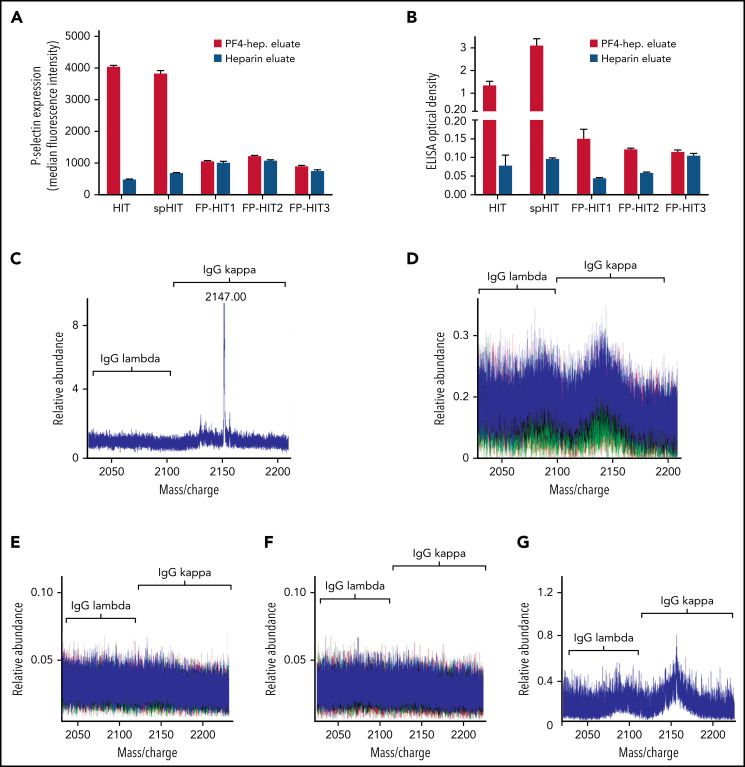
Anti-PF4 antibody characterization in spHIT, HIT, and patients with ELISA-positive but non-activating anti-PF4 antibodies (FP-HIT). (A-B) Eluates from PF4-heparin beads and control heparin beads were evaluated for platelet activation in the PEA and PF4-polyanion ELISA. Means and SD (n = 3) are shown. (C-F) Shown are LC-ESI-QTOF MS +11 light chain distributions from anti-PF4 antibodies isolated from patients with (C) spHIT, (D) HIT, and (E-G) FP-HIT. In the spectra, green represents the distribution of all λ-containing Ig’s, red represents the distribution of all κ-containing Ig’s, and blue represents the light chain distribution of κ and λ light chains associated with an IgG heavy chain. The numbers listed above peaks depict the identified light chain’s m/z ratio. The x-axis shows m/z ratios, and the y-axis depicts the relative abundance of the monoclonal or oligoclonal antibody identified.
Update of
-
Anti-PF4 VITT antibodies are oligoclonal and variably inhibited by heparin.medRxiv [Preprint]. 2021 Sep 24:2021.09.23.21263047. doi: 10.1101/2021.09.23.21263047. medRxiv. 2021. Update in: Blood. 2022 Jul 7;140(1):73-77. doi: 10.1182/blood.2021014588. PMID: 34611669 Free PMC article. Updated. Preprint.
References
-
- Creech CB, Walker SC, Samuels RJ. SARS-CoV-2 vaccines. JAMA. 2021;325(13):1318-1320. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
