

Multimorbidity, guideline-directed medical therapies, and associated outcomes among hospitalized heart failure patients
- PMID: 35561100
- PMCID: PMC9288806
- DOI: 10.1002/ehf2.13954
Multimorbidity, guideline-directed medical therapies, and associated outcomes among hospitalized heart failure patients
Abstract
Aims: Multimorbidity is common among heart failure (HF) patients and may attenuate guideline-directed medical therapy (GDMT). Multimorbid patients are under-represented in clinical trials; therefore, the effect of multimorbidity clustering on the prognosis of HF patients remains unknown. We evaluated the prevalence of multimorbidity clusters among consecutively registered hospitalized HF patients and assessed whether GDMT attenuated outcomes.
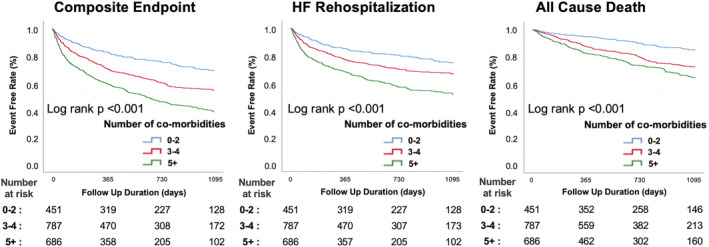
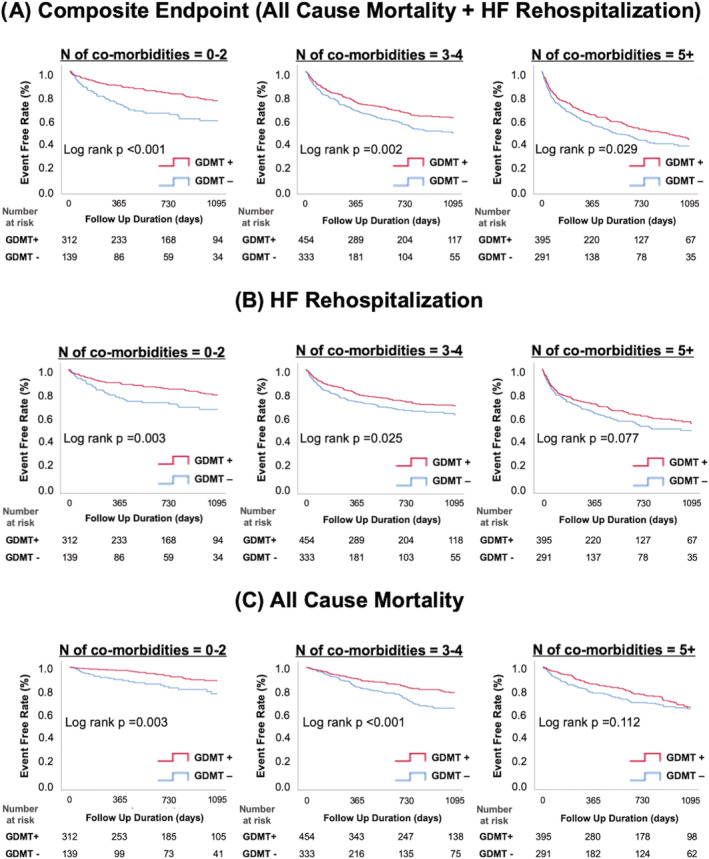
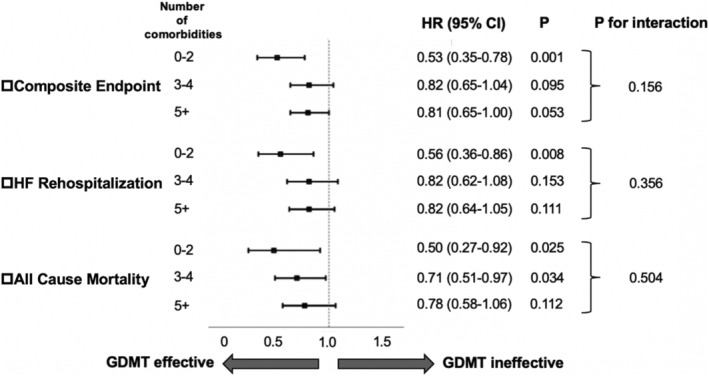
Methods and results: We examined 1924 hospitalized HF patients with reduced left ventricular ejection fraction (<50%) in a multicentre registry (West Tokyo HF Registry: WET-HF). Ten comorbid conditions in the WET-HF were abstracted: coronary artery disease, atrial fibrillation, stroke, anaemia, chronic obstructive pulmonary disease, renal dysfunction, obesity, hypertension, dyslipidaemia, and diabetes. Patients were divided into three groups (0-2: n = 451; 3-4: n = 787; and ≥5: n = 686) based on the number of comorbid conditions. The primary composite endpoint was all-cause mortality and HF rehospitalization. The most prevalent comorbidities were renal dysfunction (67.9%), hypertension (66.0%), and anaemia (53.8%). Increased comorbidity was associated with increased adverse outcomes [3-4: hazard ratio (HR) 1.42, 95% confidence interval (CI) 1.13-1.77, P = 0.003; ≥5: HR 2.12, 95%CI 1.69-2.65, P < 0.001; and reference: 0-2] and lower GDMT prescription rate (0-2: 69.2%; 3-4: 57.7%; and ≥5: 57.6%). GDMT was associated with decreased adverse outcomes; this association was maintained even as the comorbidity burden increased but tended to weaken (0-2: HR 0.53, 95%CI 0.35-0.78; P = 0.001; 3-4: HR 0.82, 95%CI 0.65-1.04, P = 0.095; and ≥5: HR 0.81, 95%CI 0.65-1.00, P = 0.053; P for interaction = 0.156).
Conclusions: Comorbidity clusters were prevalent and associated with poorer outcomes. GDMT remained beneficial regardless of the comorbidity burden but tended to weaken with increasing comorbidity burden. Further research is required to optimize medical care in these patients.
Keywords: Comorbidity; Guideline-directed medical therapy; Heart failure; Multimorbidity.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Y.S. is affiliated with an endowed department that is supported by Nippon Shinyaku Co., Ltd., has received a research grant from the SECOM Science and Technology Foundation, and has received an honorarium from Otsuka Pharmaceutical Co., Ltd. S.K. has received an unrestricted research grant from the Department of Cardiology, Keio University School of Medicine, Bayer Pharmaceutical Co., Ltd., and Daiichi Sankyo Co., Ltd. S.T. has received a research grant from the Bayer Pharmaceutical Co., Ltd. The remaining authors have no conflicts of interest to disclose. There are no patents, products in development, or marketed products to declare.
Figures

Similar articles
-
Low blood pressure and guideline-directed medical therapy in patients with heart failure with reduced ejection fraction.Int J Cardiol. 2023 Jan 1;370:255-262. doi: 10.1016/j.ijcard.2022.10.129. Epub 2022 Oct 19. Int J Cardiol. 2023. PMID: 36270494
-
The role of multimorbidity in patients with heart failure across the left ventricular ejection fraction spectrum: Data from the Swedish Heart Failure Registry.Eur J Heart Fail. 2024 Apr;26(4):854-868. doi: 10.1002/ejhf.3112. Epub 2024 Jan 8. Eur J Heart Fail. 2024. PMID: 38131248
-
Impact of multimorbidity on mortality in heart failure with reduced ejection fraction: which comorbidities matter most? An analysis of PARADIGM-HF and ATMOSPHERE.Eur J Heart Fail. 2023 May;25(5):687-697. doi: 10.1002/ejhf.2856. Epub 2023 Apr 24. Eur J Heart Fail. 2023. PMID: 37062869
-
Relationship between comorbidity and health outcomes in patients with heart failure: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2023 Oct 10;23(1):498. doi: 10.1186/s12872-023-03527-x. BMC Cardiovasc Disord. 2023. PMID: 37817062 Free PMC article.
-
Navigating between Scylla and Charybdis: challenges and strategies for implementing guideline-directed medical therapy in heart failure with reduced ejection fraction.Eur J Heart Fail. 2021 Dec;23(12):1999-2007. doi: 10.1002/ejhf.2378. Epub 2021 Dec 13. Eur J Heart Fail. 2021. PMID: 34755422 Review.
Cited by
-
Medication-focused telehealth interventions to reduce the hospital readmission rate: a systematic review.J Pharm Policy Pract. 2025 Feb 5;18(1):2457411. doi: 10.1080/20523211.2025.2457411. eCollection 2025. J Pharm Policy Pract. 2025. PMID: 39917474 Free PMC article. Review.
-
Risk prediction models for mortality in patients with multimorbidity: a systematic review and meta-analysis.Front Public Health. 2025 Apr 2;13:1505541. doi: 10.3389/fpubh.2025.1505541. eCollection 2025. Front Public Health. 2025. PMID: 40241941 Free PMC article.
-
Therapeutic Consequences and Prognostic Impact of Multimorbidity in Heart Failure: Time to Act.J Clin Med. 2024 Dec 29;14(1):139. doi: 10.3390/jcm14010139. J Clin Med. 2024. PMID: 39797222 Free PMC article.
-
Rationale and protocol of the LAQUA-HF trial: a factorial randomised controlled trial evaluating the effects of neurohormonal and diuretic agents on health-status reported outcomes in heart failure patients.BMJ Open. 2024 Feb 14;14(2):e076519. doi: 10.1136/bmjopen-2023-076519. BMJ Open. 2024. PMID: 38355194 Free PMC article.
-
High-intensity care for GDMT titration.Heart Fail Rev. 2024 Sep;29(5):1065-1077. doi: 10.1007/s10741-024-10419-5. Epub 2024 Jul 22. Heart Fail Rev. 2024. PMID: 39037564 Free PMC article. Review.
References
-
- Murphy SP, Ibrahim NE, Januzzi JL Jr. Heart failure with reduced ejection fraction: a review. JAMA. 2020; 324: 488–504. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJV, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WHW, Tsai EJ, Wilkoff BL. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013; 128: 1810–1852. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P, Authors/Task Force Members , Document reviewers . 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016; 18: 891–975. - PubMed
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo‐Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano GMC, Ruschitzka F, Kathrine Skibelund A, ESC Scientific Document Group , de Boer RA, Christian Schulze P, Abdelhamid M, Aboyans V, Adamopoulos S, Anker SD, Arbelo E, Asteggiano R, Bauersachs J, Bayes‐Genis A, Borger MA, Budts W, Cikes M, Damman K, Delgado V, Dendale P, Dilaveris P, Drexel H, Ezekowitz J, Falk V, Fauchier L, Filippatos G, Fraser A, Frey N, Gale CP, Gustafsson F, Harris J, Iung B, Janssens S, Jessup M, Konradi A, Kotecha D, Lambrinou E, Lancellotti P, Landmesser U, Leclercq C, Lewis BS, Leyva F, Linhart A, Løchen ML, Lund LH, Mancini D, Masip J, Milicic D, Mueller C, Nef H, Nielsen JC, Neubeck L, Noutsias M, Petersen SE, Sonia Petronio A, Ponikowski P, Prescott E, Rakisheva A, Richter DJ, Schlyakhto E, Seferovic P, Senni M, Sitges M, Sousa‐Uva M, Tocchetti CG, Touyz RM, Tschoepe C, Waltenberger J, Adamo M, Baumbach A, Böhm M, Burri H, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo‐Leiro MG, Farmakis D, Gardner RS, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Piepoli MF, Price S, Rosano GMC, Ruschitzka F, Skibelund AK. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42: 3599–3726. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
