

SARS-CoV-2 RNA and antibody dynamics in a Dutch household study with dense sampling frame
- PMID: 35562380
- PMCID: PMC9099349
- DOI: 10.1038/s41598-022-11480-6
SARS-CoV-2 RNA and antibody dynamics in a Dutch household study with dense sampling frame
Abstract
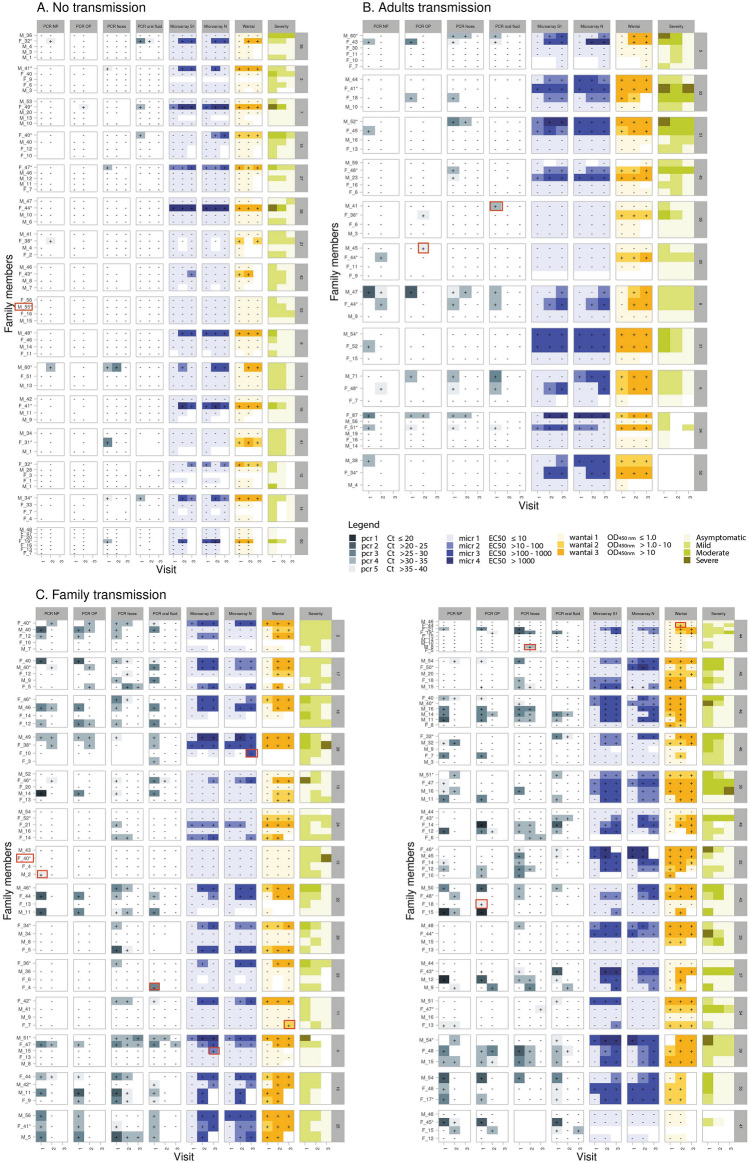
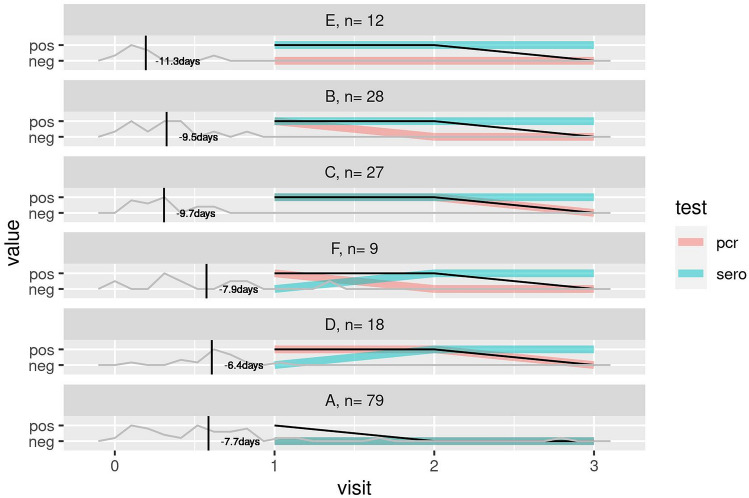
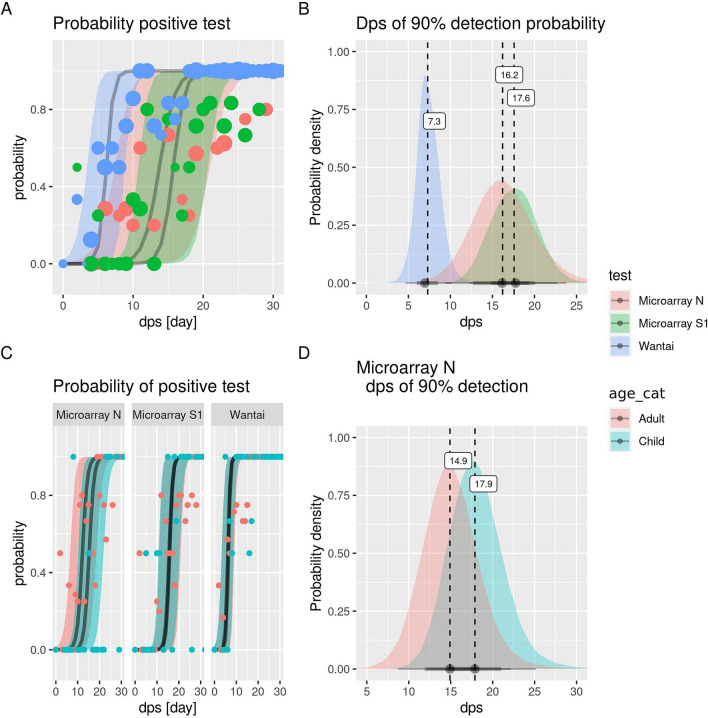
This study investigated the dynamics of SARS-CoV-2 infection and diagnostics in 242 household members of different ages and with different symptom severity after SARS-CoV-2 exposure early in the pandemic (March-April 2020). Households with a SARS-CoV-2 confirmed positive case and at least one child in the Netherlands were followed for 6 weeks. Naso (NP)- and oropharyngeal (OP) swabs, oral fluid and feces specimens were analyzed for SARS-CoV-2 RNA and serum for SARS-CoV-2-specific antibodies. The dynamics of the presence of viral RNA and the serological response was modeled to determine the sampling time-frame and sample type with the highest sensitivity to confirm or reject a SARS-CoV-2 diagnosis. In children higher viral loads compared to adults were detected at symptom onset. Early in infection, higher viral loads were detected in NP and OP specimens, while RNA in especially feces were longer detectable. SARS-CoV-2-specific antibodies have 90% probability of detection from 7 days (total Ig) and 18 days (IgG) since symptom onset. For highest probability of detection in SARS-CoV-2 diagnostics early in infection, RT-PCR on NP and OP specimens are more sensitive than on oral fluid and feces. For SARS-CoV-2 diagnostics late after infection, RT-PCR on feces specimens and serology are more valuable.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- World Health Organization (WHO). Timeline of WHO's response to COVID-19. https://www.who.int/news/item/29-06-2020-covidtimeline.
-
- Minister Bruno Bruins MIvE, Minister Arie Slob, Minister Tamara van Ark. Kamerbrief met nieuwe aanvullende maatregelen om de COVID 19 uitbraak te bestrijden. Medische Zorg en Sport OCeW, Basis- en Voortgezet Onderwijs en Media, Sociale Zaken en Werkgelegenheid. Den Haag, 15 March 2020.
-
- WHO. Clinical management of COVID-19 (2020).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
