

Genomic architecture of fetal central nervous system anomalies using whole-genome sequencing
- PMID: 35562572
- PMCID: PMC9106651
- DOI: 10.1038/s41525-022-00301-4
Genomic architecture of fetal central nervous system anomalies using whole-genome sequencing
Abstract
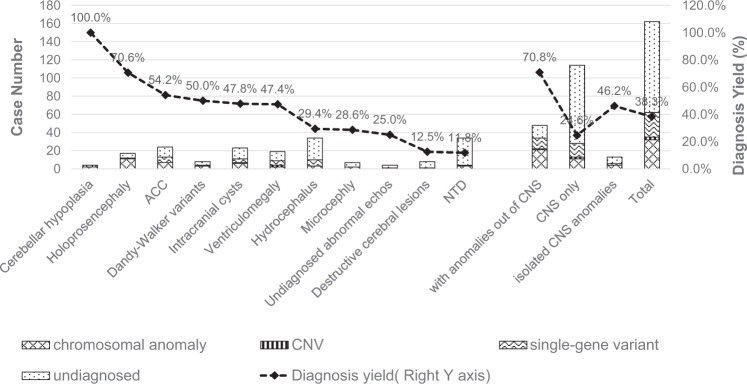
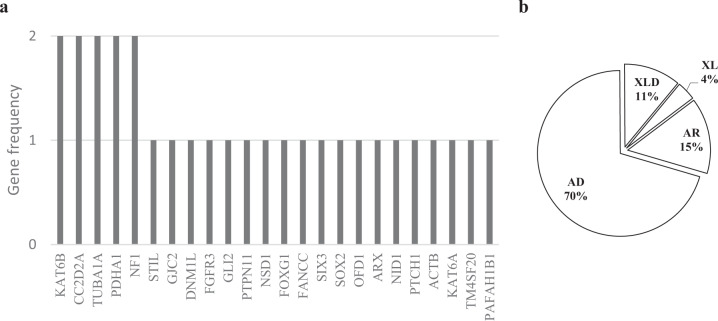
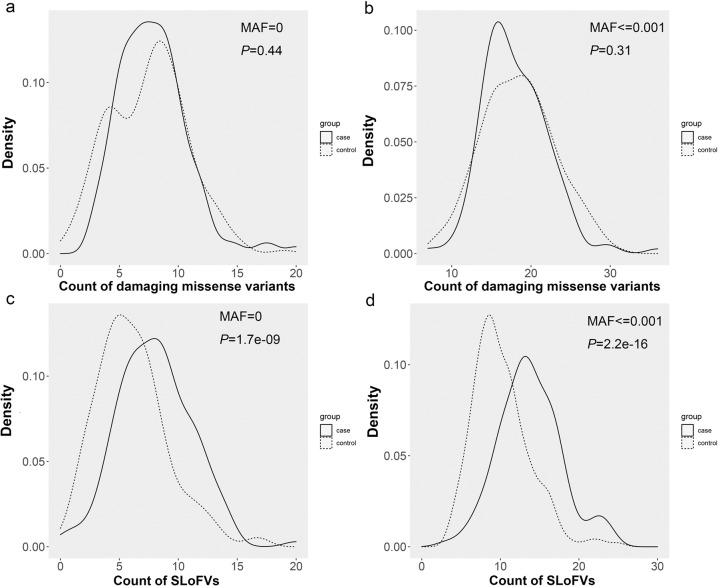
Structural anomalies of the central nervous system (CNS) are one of the most common fetal anomalies found during prenatal imaging. However, the genomic architecture of prenatal imaging phenotypes has not yet been systematically studied in a large cohort. Patients diagnosed with fetal CNS anomalies were identified from medical records and images. Fetal samples were subjected to low-pass and deep whole-genome sequencing (WGS) for aneuploid, copy number variation (CNV), single-nucleotide variant (SNV, including insertions/deletions (indels)), and small CNV identification. The clinical significance of variants was interpreted based on a candidate gene list constructed from ultrasound phenotypes. In total, 162 fetuses with 11 common CNS anomalies were enrolled in this study. Primary diagnosis was achieved in 62 cases, with an overall diagnostic rate of 38.3%. Causative variants included 18 aneuploids, 17 CNVs, three small CNVs, and 24 SNVs. Among the 24 SNVs, 15 were novel mutations not reported previously. Furthermore, 29 key genes of diagnostic variants and critical genes of pathogenic CNVs were identified, including five recurrent genes: i.e., TUBA1A, KAT6B, CC2D2A, PDHA1, and NF1. Diagnostic variants were present in 34 (70.8%) out of 48 fetuses with both CNS and non-CNS malformations, and in 28 (24.6%) out of 114 fetuses with CNS anomalies only. Hypoplasia of the cerebellum (including the cerebellar vermis) and holoprosencephaly had the highest primary diagnosis yields (>70%), while only four (11.8%) out of 34 neural tube defects achieved genetic diagnosis. Compared with the control group, rare singleton loss-of-function variants (SLoFVs) were significantly accumulated in the patient cohort.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- International Society of Ultrasound in, O. & Gynecology Education, C. Sonographic examination of the fetal central nervous system: guidelines for performing the ‘basic examination’ and the ‘fetal neurosonogram’. Ultrasound Obstet. Gynecol.29, 109–116 (2007). - PubMed
-
- Paladini D, et al. Accuracy of neurosonography and MRI in clinical management of fetuses referred with central nervous system abnormalities. Ultrasound Obstet. Gynecol. 2014;44:188–196. - PubMed
Grants and funding
- WJ2018H0132/Health and Family Planning Commission of Hubei Province (Hubei Provincial Health Department)
- WJ2018H0141/Health and Family Planning Commission of Hubei Province (Hubei Provincial Health Department)
- ZRMS2017001139/Natural Science Foundation of Hubei Province (Hubei Provincial Natural Science Foundation)
- JCYJ20180703093402288/Shenzhen Science and Technology Innovation Commission
- No. 2019B020227001/Guangdong Science and Technology Department (Science and Technology Department, Guangdong Province)
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
