

Anemia and adverse outcomes in pregnancy: subgroup analysis of the CLIP cluster-randomized trial in India
- PMID: 35562720
- PMCID: PMC9101819
- DOI: 10.1186/s12884-022-04714-y
Anemia and adverse outcomes in pregnancy: subgroup analysis of the CLIP cluster-randomized trial in India
Abstract
Background: Iron-deficiency anemia is a known risk factor for several adverse perinatal outcomes, but data on its impact on specific maternal morbidities is less robust. Further, information on associations between anemia in early pregnancy and subsequent outcomes are understudied.
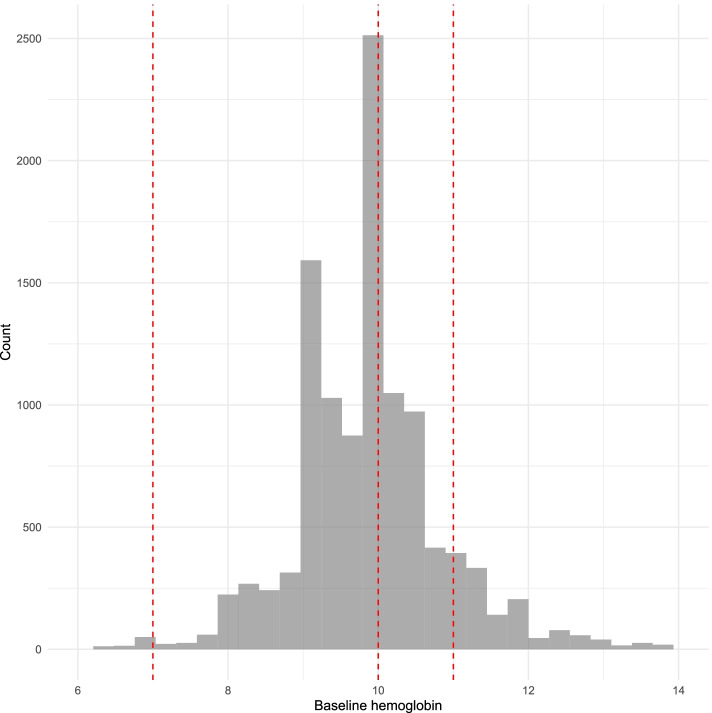
Methods: The study population was derived from the Community Level Interventions for Pre-eclampsia (CLIP) trial in Karnataka State, India (NCT01911494). Included were women who were enrolled in either trial arm, delivered by trial end date, and had a baseline measure of hemoglobin (Hb). Anemia was classified by WHO standards into four groups: none (Hb ≥ 11 g/dL), mild (10.0 g/dL ≤ Hb < 11.0 g/dL), moderate (7.0 g/dL ≤ Hb < 10.0 g/dL) and severe (Hb < 7.0 g/dL). Targeted maximum likelihood estimation was used to estimate confounder-adjusted associations between anemia and a composite (and its components) of adverse maternal outcomes, including pregnancy hypertension. E-values were calculated to assess robustness to unmeasured confounding.
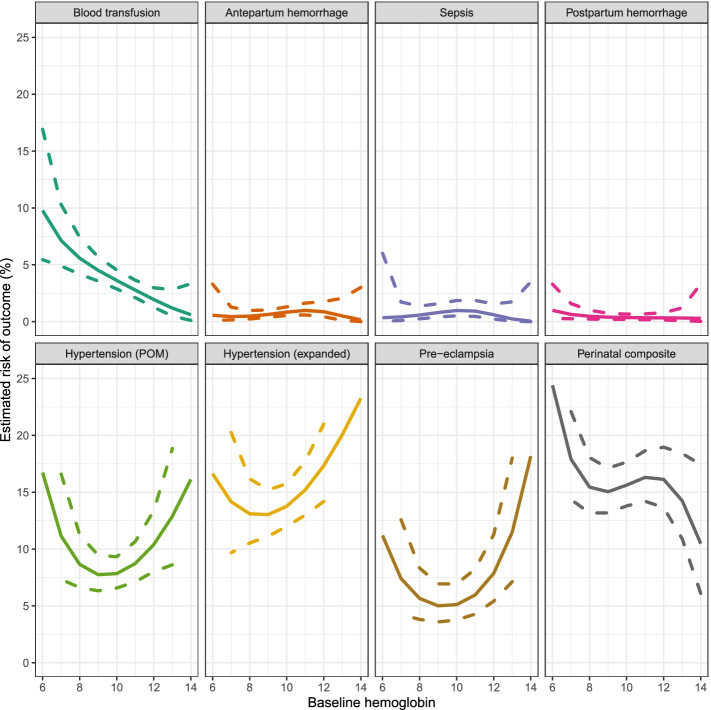
Results: Of 11,370 women included, 10,066 (88.5%) had anemia, that was mild (3690, 32.5%), moderate (6023, 53.0%), or severe (68, 0.6%). Almost all women (> 99%) reported taking iron supplements during pregnancy. Blood transfusions was more often administered to those with anemia that was mild (risk ratio [RR] 2.16, 95% confidence interval [CI] 1.31-3.56), moderate (RR 2.37, 95% CI 1.56-3.59), and severe (RR 5.70, 95% CI 3.00-10.85). No significant association was evident between anemia severity and haemorrhage (antepartum or postpartum) or sepsis, but there was a U-shaped association between anemia severity and pregnancy hypertension and pre-eclampsia specifically, with the lowest risk seen among those with mild or moderate anemia.
Conclusion: In Karnataka State, India, current management strategies for mild-moderate anemia in early pregnancy are associated with similar rates of adverse maternal or perinatal outcomes, and a lower risk of pregnancy hypertension and preeclampsia, compared with no anemia in early pregnancy. Future research should focus on risk mitigation for women with severe anemia, and the potential effect of iron supplementation for women with normal Hb in early pregnancy.
Keywords: Anemia in pregnancy; Global health; Hypertension.
© 2022. The Author(s).
Conflict of interest statement
LAM and PvD report grants from the Bill & Melinda Gates Foundation, during the conduct of the study. All other authors declare no competing interests.
Figures
References
-
- Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Glob Health. 2013;1(1):e16–25. doi: 10.1016/S2214-109X(13)70001-9. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
