

Repair of acute respiratory distress syndrome by stromal cell administration (REALIST): a structured study protocol for an open-label dose-escalation phase 1 trial followed by a randomised, triple-blind, allocation concealed, placebo-controlled phase 2 trial
- PMID: 35562778
- PMCID: PMC9099345
- DOI: 10.1186/s13063-022-06220-0
Repair of acute respiratory distress syndrome by stromal cell administration (REALIST): a structured study protocol for an open-label dose-escalation phase 1 trial followed by a randomised, triple-blind, allocation concealed, placebo-controlled phase 2 trial
Abstract
Background: Mesenchymal stromal cells (MSCs) may be of benefit in ARDS due to immunomodulatory and reparative properties. This trial investigates a novel CD362 enriched umbilical cord derived MSC product (REALIST ORBCEL-C), produced to Good Manufacturing Practice standards, in patients with moderate to severe ARDS due to COVID-19 and ARDS due to other causes.
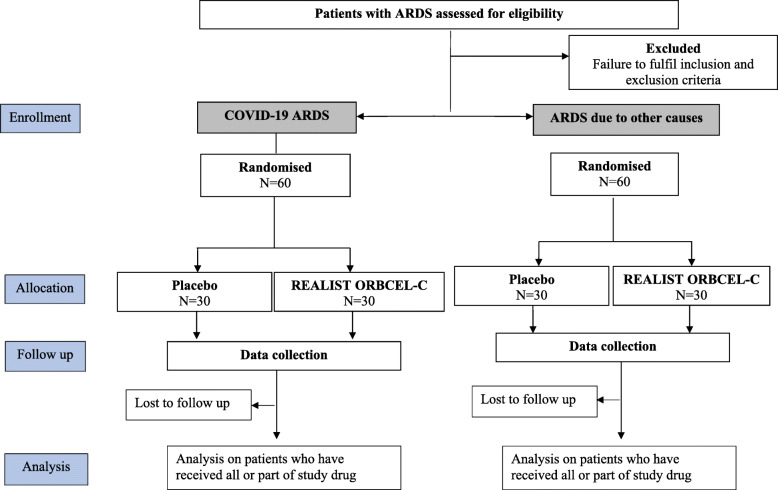
Methods: Phase 1 is a multicentre open-label dose-escalation pilot trial. Patients will receive a single infusion of REALIST ORBCEL-C (100 × 106 cells, 200 × 106 cells or 400 × 106 cells) in a 3 + 3 design. Phase 2 is a multicentre randomised, triple blind, allocation concealed placebo-controlled trial. Two cohorts of patients, with ARDS due to COVID-19 or ARDS due to other causes, will be recruited and randomised 1:1 to receive either a single infusion of REALIST ORBCEL-C (400 × 106 cells or maximal tolerated dose in phase 1) or placebo. Planned recruitment to each cohort is 60 patients. The primary safety outcome is the incidence of serious adverse events. The primary efficacy outcome is oxygenation index at day 7. The trial will be reported according to the Consolidated Standards for Reporting Trials (CONSORT 2010) statement.
Discussion: The development and manufacture of an advanced therapy medicinal product to Good Manufacturing Practice standards within NHS infrastructure are discussed, including challenges encountered during the early stages of trial set up. The rationale to include a separate cohort of patients with ARDS due to COVID-19 in phase 2 of the trial is outlined.
Trial registration: ClinicalTrials.gov NCT03042143. Registered on 3 February 2017. EudraCT Number 2017-000584-33.
Keywords: Acute respiratory distress syndrome; COVID-19; Clinical trial; MSCs; Mesenchymal stem cells; Mesenchymal stromal cells; Protocol.
© 2022. The Author(s).
Conflict of interest statement
EG receives funding by the Wellcome Trust Health Innovation Challenge Fund [reference 106939/Z/15/Z] for the described work. COK, DMcA, JL and JS are investigators on the grant funding this work from Wellcome Trust Health Innovation Challenge Fund [reference 106939/Z/15/Z]. DMcA, COK and MC are investigators on a grant received from the Northern Ireland Health and Social Care Research and Development Division to fund an additional COVID-19 cohort during phase 2 of the REALIST trial
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23) 10.1001/jama.2012.5669. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley D, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, LUNG SAFE Investigators. ESICM Trials Group Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Bienvenu OJ, Friedman LA, Colantuoni E, Dinglas VD, Sepulveda KA, Mendez-Tellez P, Shanholz C, Pronovost PJ, Needham DM. Psychiatric symptoms after acute respiratory distress syndrome: a 5-year longitudinal study. Intensive Care Med. 2018;44(1):38–47. doi: 10.1007/s00134-017-5009-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
