

Primary Aldosteronism and Resistant Hypertension: A Pathophysiological Insight
- PMID: 35563192
- PMCID: PMC9100181
- DOI: 10.3390/ijms23094803
Primary Aldosteronism and Resistant Hypertension: A Pathophysiological Insight
Abstract
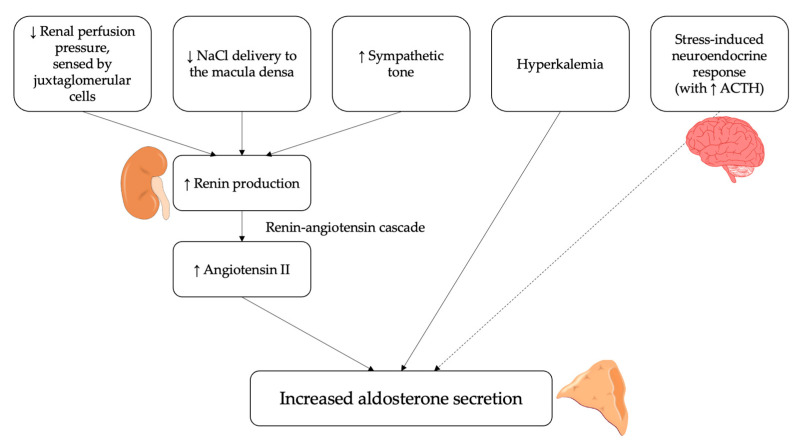
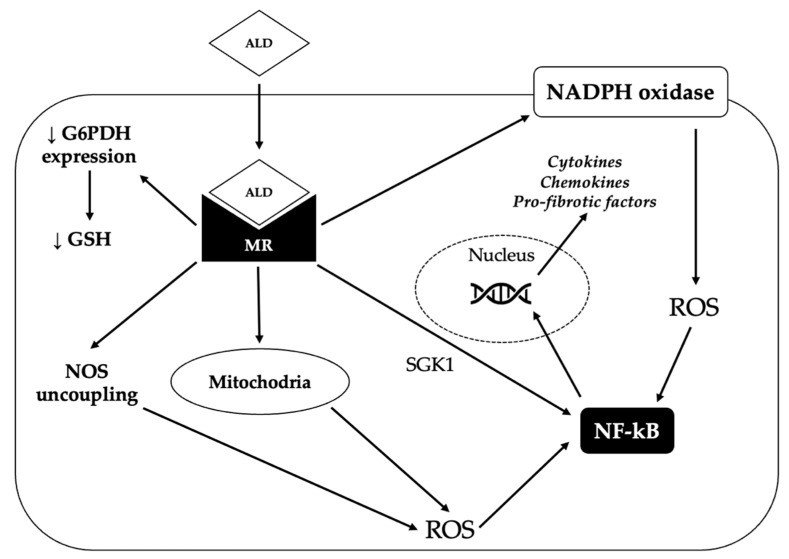
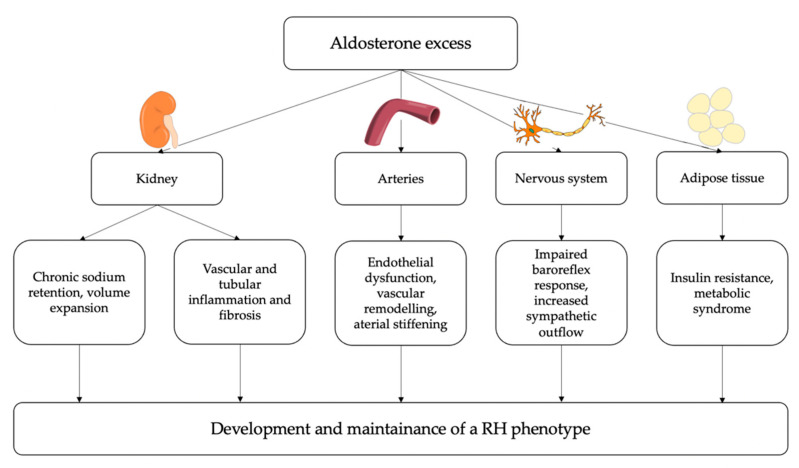
Primary aldosteronism (PA) is a pathological condition characterized by an excessive aldosterone secretion; once thought to be rare, PA is now recognized as the most common cause of secondary hypertension. Its prevalence increases with the severity of hypertension, reaching up to 29.1% in patients with resistant hypertension (RH). Both PA and RH are "high-risk phenotypes", associated with increased cardiovascular morbidity and mortality compared to non-PA and non-RH patients. Aldosterone excess, as occurs in PA, can contribute to the development of a RH phenotype through several mechanisms. First, inappropriate aldosterone levels with respect to the hydro-electrolytic status of the individual can cause salt retention and volume expansion by inducing sodium and water reabsorption in the kidney. Moreover, a growing body of evidence has highlighted the detrimental consequences of "non-classical" effects of aldosterone in several target tissues. Aldosterone-induced vascular remodeling, sympathetic overactivity, insulin resistance, and adipose tissue dysfunction can further contribute to the worsening of arterial hypertension and to the development of drug-resistance. In addition, the pro-oxidative, pro-fibrotic, and pro-inflammatory effects of aldosterone may aggravate end-organ damage, thereby perpetuating a vicious cycle that eventually leads to a more severe hypertensive phenotype. Finally, neither the pathophysiological mechanisms mediating aldosterone-driven blood pressure rise, nor those mediating aldosterone-driven end-organ damage, are specifically blocked by standard first-line anti-hypertensive drugs, which might further account for the drug-resistant phenotype that frequently characterizes PA patients.
Keywords: aldosterone; arterial hypertension; pathophysiology; primary aldosteronism; resistant hypertension; secondary hypertension.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Parasiliti-Caprino M., Lopez C., Prencipe N., Lucatello B., Settanni F., Giraudo G., Rossato D., Mengozzi G., Ghigo E., Benso A., et al. Prevalence of Primary Aldosteronism and Association with Cardiovascular Complications in Patients with Resistant and Refractory Hypertension. J. Hypertens. 2020;38:1841–1848. doi: 10.1097/HJH.0000000000002441. - DOI - PubMed
-
- Monticone S., D’Ascenzo F., Moretti C., Williams T.A., Veglio F., Gaita F., Mulatero P. Cardiovascular Events and Target Organ Damage in Primary Aldosteronism Compared with Essential Hypertension: A Systematic Review and Meta-Analysis. Lancet Diabetes Endocrinol. 2018;6:41–50. doi: 10.1016/S2213-8587(17)30319-4. - DOI - PubMed
