

Effects of One-Day Application of Levodopa/Carbidopa/Entacapone versus Levodopa/Carbidopa/Opicapone in Parkinson's Disease Patients
- PMID: 35563817
- PMCID: PMC9105632
- DOI: 10.3390/cells11091511
Effects of One-Day Application of Levodopa/Carbidopa/Entacapone versus Levodopa/Carbidopa/Opicapone in Parkinson's Disease Patients
Abstract
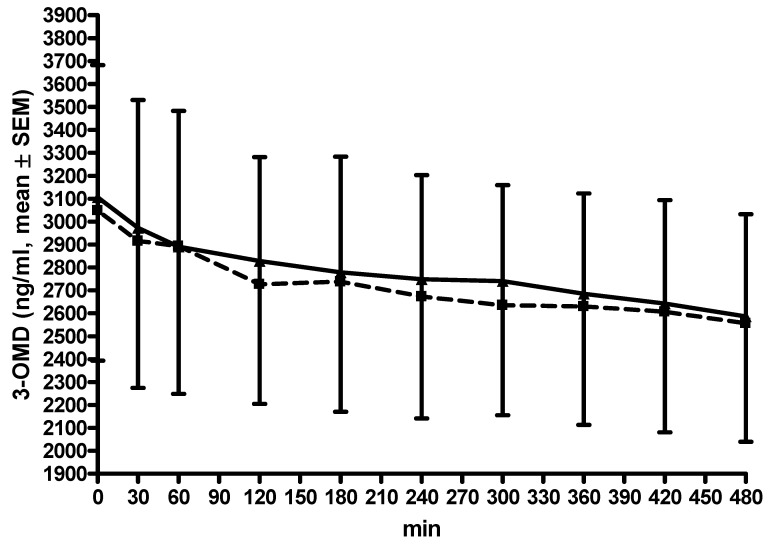
The catechol-O-methyltransferase inhibitors entacapone and opicapone prolong the efficacy of conventional oral levodopa/dopa decarboxylase inhibitor formulations through an increase in levodopa plasma bioavailability. Catechol-O-methyltransferase inhibitors influence the homocysteine metabolism associated with levodopa/dopa decarboxylase application. The objectives of this study were to compare the impact of additional single-day entacapone or opicapone intake on the pharmacokinetic plasma behaviour of levodopa, 3-O-methyldopa and total homocysteine in 15 Parkinson's disease patients, with concomitant scoring of motor symptoms, under standardized conditions. The patients received opicapone plus two doses of 100 mg levodopa/carbidopa and, one week later, two doses of levodopa/carbidopa/entacapone or vice versa. Levodopa, 3-O-methyldopa and total homocysteine were determined with reversed-phase high-performance liquid chromatography. Levodopa bioavailability and its maximum concentration were higher with opicapone. The computed peak-to-trough difference was lower after the second levodopa administration with entacapone. The fluctuation index of levodopa did not differ between both conditions. 3-O-methyldopa decreased on both days. Homocysteine levels did not significantly vary between both conditions. A significant homocysteine decrease occurred with entacapone, but not with opicapone. Motor behaviour improved with entacapone, but not with opicapone. Opicapone baseline scores were significantly better, and thus the potential for the improvement in motor symptoms was lower compared with the entacapone condition. The higher levodopa bioavailability with opicapone suggests that it is more efficacious than entacapone for the amelioration of "off" phenomena in fluctuating patients when co-administered with a levodopa/dopa decarboxylase inhibitor regimen. Both compounds prevented an increase in homocysteine, which is a metabolic marker for an impaired capacity in the performance of methylation processes.
Keywords: 3-O-methyldopa; Parkinson’s disease; entacapone; homocysteine; levodopa; opicapone.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Fahn S., Oakes D., Shoulson I., Kieburtz K., Lang A.E., Olanow C.W., Tanner C.M., Marek K. Levodopa and the progression of Parkinson’s disease. N. Engl. J. Med. 2004;351:2498–2508. - PubMed
-
- Ferreira J.J., Lees A., Rocha J.F., Poewe W., Rascol O., Soares-da-Silva P. Long-term efficacy of opicapone in fluctuating Parkinson’s disease patients: A pooled analysis of data from two phase 3 clinical trials and their open-label extensions. Eur. J. Neurol. 2019;26:953–960. doi: 10.1111/ene.13914. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
