

COVID-19 Clinical Profiles and Fatality Rates in Hospitalized Patients Reveal Case Aggravation and Selective Co-Infection by Limited Gram-Negative Bacteria
- PMID: 35564665
- PMCID: PMC9101447
- DOI: 10.3390/ijerph19095270
COVID-19 Clinical Profiles and Fatality Rates in Hospitalized Patients Reveal Case Aggravation and Selective Co-Infection by Limited Gram-Negative Bacteria
Abstract
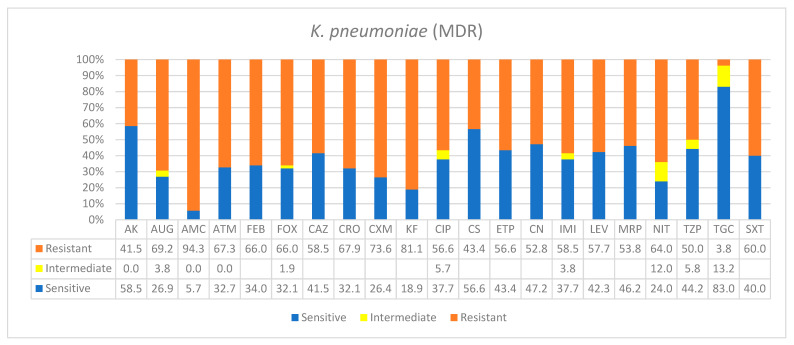
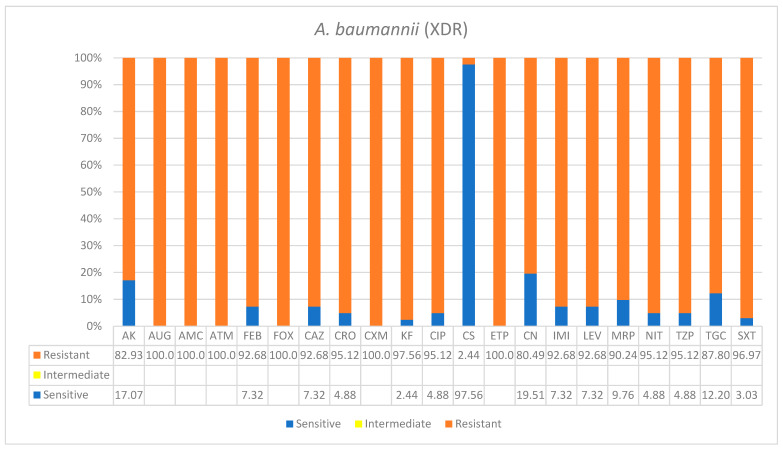
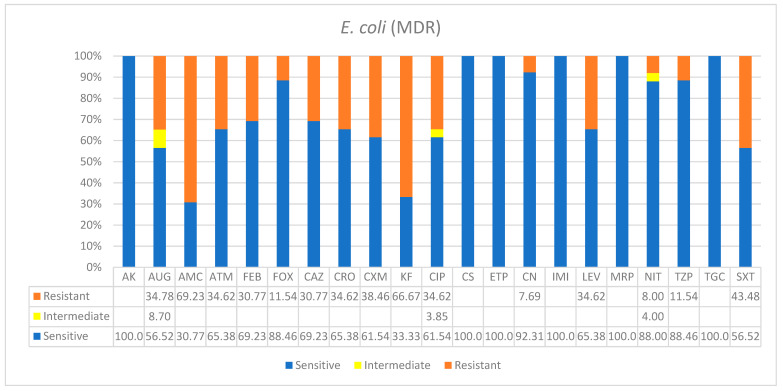
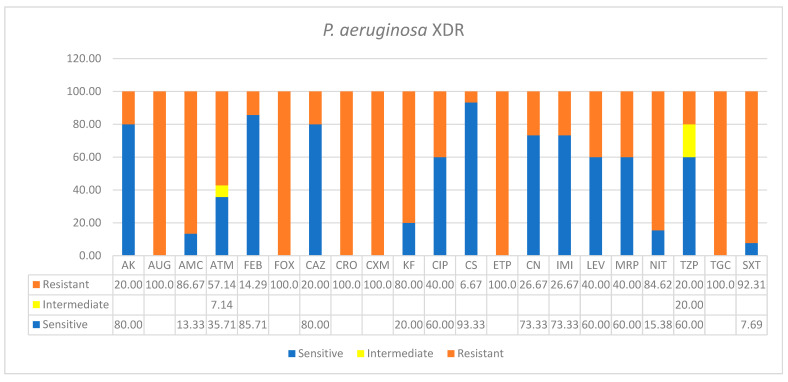
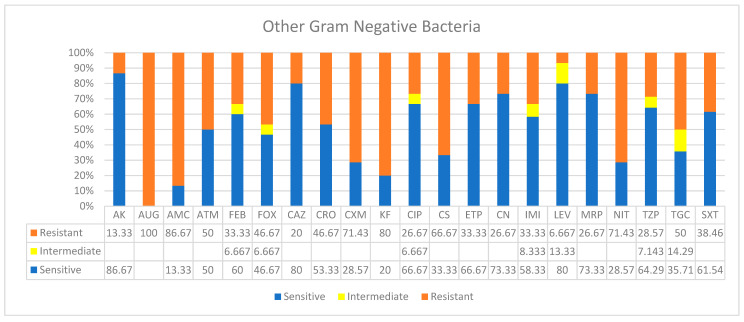
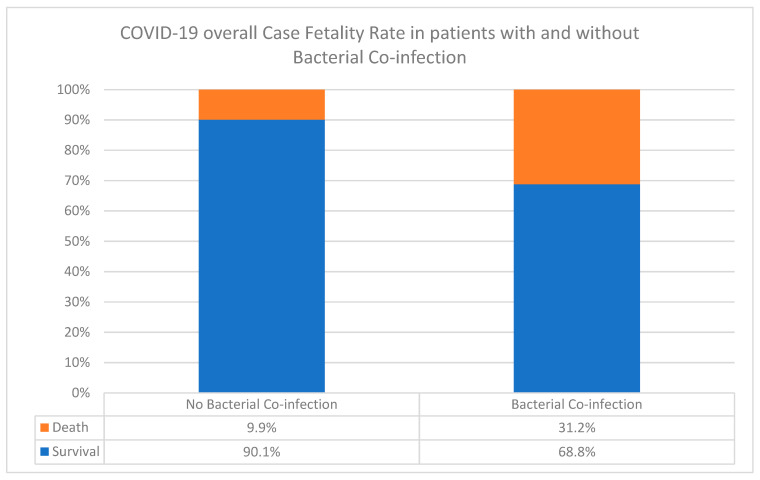
Bacterial co-infections may aggravate COVID-19 disease, and therefore being cognizant of other pathogens is imperative. We studied the types, frequency, antibiogram, case fatality rates (CFR), and clinical profiles of co-infecting-pathogens in 301 COVID-19 patients. Co-infection was 36% (n = 109), while CFR was 31.2% compared to 9.9% in non-co-infected patients (z-value = 3.1). Four bacterial species dominated, namely, multidrug-resistant Klebsiella pneumoniae (37%, n = 48), extremely drug-resistant Acinetobacter baumannii (26%, n = 34), multidrug-resistant Eschericia. coli (18.6%, n = 24), and extremely drug-resistant Pseudomonas aeruginosa (8.5%, n = 11), in addition to other bacterial species (9.3%, n = 12). Increased co-infection of K. pneumoniae and A. baumannii was associated with increased death rates of 29% (n = 14) and 32% (n = 11), respectively. Klebsiella pneumoniae was equally frequent in respiratory and urinary tract infections (UTI), while E. coli mostly caused UTI (67%), and A. baumannii and P. aeruginosa dominated respiratory infections (38% and 45%, respectively). Co-infections correlated with advance in age: seniors ≥ 50 years (71%), young adults 21-49 years (25.6%), and children 0-20 years (3%). These findings have significant clinical implications in the successful COVID-19 therapies, particularly in geriatric management. Future studies would reveal insights into the potential selective mechanism(s) of Gram-negative bacterial co-infection in COVID-19 patients.
Keywords: SARS-CoV-2 pandemic; empirical-antimicrobial therapy; mortality; nosocomial resistance; selective infections.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Wu Y., Tu W., Lam K.-T., Chow K.-H., Ho P.-L., Guan Y., Peiris J.S.M., Lau Y.-L. Lethal Coinfection of Influenza Virus and Streptococcus Pneumoniae Lowers Antibody Response to Influenza Virus in Lung and Reduces Numbers of Germinal Center B Cells, T Follicular Helper Cells, and Plasma Cells in Mediastinal Lymph Node. J. Virol. 2015;89:2013–2023. doi: 10.1128/JVI.02455-14. - DOI - PMC - PubMed
-
- Garcia-Vidal C., Viasus D., Roset A., Adamuz J., Verdaguer R., Dorca J., Gudiol F., Carratalà J. Low Incidence of Multidrug-Resistant Organisms in Patients with Healthcare-Associated Pneumonia Requiring Hospitalization. Clin. Microbiol. Infect. 2011;17:1659–1665. doi: 10.1111/j.1469-0691.2011.03484.x. - DOI - PubMed
-
- Chen N., Zhou M., Dong X., Qu J., Gong F., Han Y., Qiu Y., Wang J., Liu Y., Wei Y., et al. Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: A Descriptive Study. Lancet. 2020;395:507–513. doi: 10.1016/S0140-6736(20)30211-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
