

Can Surgical Resection of Metastatic Lesions Be Beneficial to Pancreatic Ductal Adenocarcinoma Patients with Isolated Lung Metastasis?
- PMID: 35565195
- PMCID: PMC9099489
- DOI: 10.3390/cancers14092067
Can Surgical Resection of Metastatic Lesions Be Beneficial to Pancreatic Ductal Adenocarcinoma Patients with Isolated Lung Metastasis?
Abstract
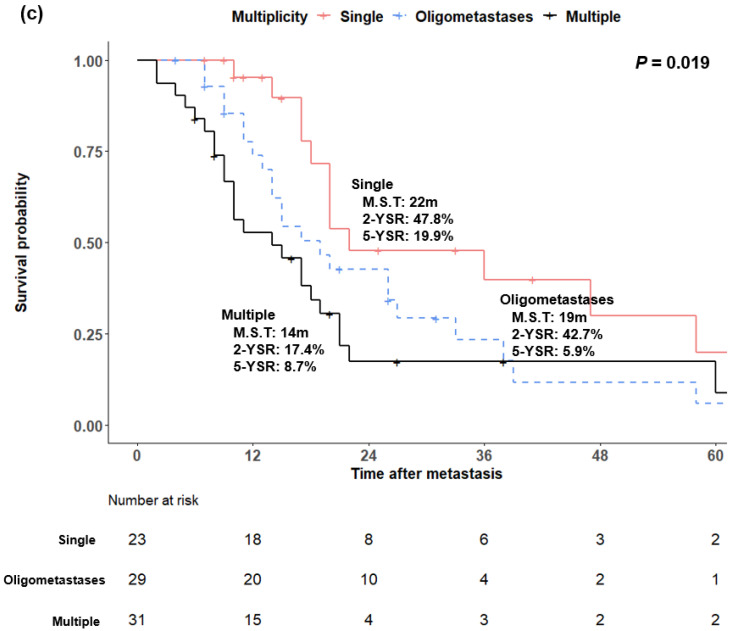
In the era of effective chemotherapy on pancreatic ductal adenocarcinoma (PDAC) with distant metastasis, data on the effects of metastatectomy are lacking. So, we investigated the effect of metastatectomy on survival after metastasis in PDAC patients with isolated lung metastasis. This retrospective study analyzed 1342 patients who were histologically diagnosed with PDAC with distant metastasis from January 2007 to December 2018, of which 83 patients had isolated pulmonary metastasis. Additionally, 4263 patients were extracted from the National Cancer Database (NCDB) and analyzed. Log-rank test and Kaplan−Meier survival analysis were used to analyze survival after metastasis. The five-year survival rate was significantly higher in patients who underwent pulmonary metastatectomy than in those who received only chemotherapy or supportive treatment (60.6% vs. 6.2% vs. 0.0%, p < 0.001). A similar trend was observed in the NCDB (two-year survival rate, 27.4% vs. 15.8% vs. 4.7%, p < 0.001). In the multivariate analysis, lung lesion multiplicity (hazard ratio (HR) = 2.004, p = 0.017), metastatectomy (HR = 0.278, p = 0.036), chemotherapy (HR = 0.434, p = 0.024), and chemotherapy cycles (HR = 0.300, p < 0.001) had significant effects on survival. Metastatectomy with primary pancreatic lesions is recommended with effective chemotherapy in PDAC patients with isolated lung metastasis.
Keywords: chemotherapy; metastasis/lung; metastatectomy; pancreatic ductal adenocarcinoma; survival.
Conflict of interest statement
All of the authors declare no competing interest.
Figures






Similar articles
-
Surgical treatment of hepatic oligometastatic pancreatic ductal adenocarcinoma: An analysis of the National Cancer Database.Surgery. 2022 Jun;171(6):1464-1470. doi: 10.1016/j.surg.2021.12.029. Epub 2022 Feb 1. Surgery. 2022. PMID: 35115154
-
Impact of Ovarian Metastatectomy on Survival Outcome of Colorectal Cancer Patients with Ovarian Metastasis: A Retrospective Study.Cancer Manag Res. 2020 Jun 12;12:4493-4501. doi: 10.2147/CMAR.S254876. eCollection 2020. Cancer Manag Res. 2020. PMID: 32606943 Free PMC article.
-
Significance of pulmonary resection in patients with metachronous pulmonary metastasis from pancreatic ductal adenocarcinoma: a retrospective cohort study.BMC Surg. 2021 May 5;21(1):237. doi: 10.1186/s12893-021-01236-w. BMC Surg. 2021. PMID: 33952223 Free PMC article.
-
Different clinical presentations of metachronous pulmonary metastases after resection of pancreatic ductal adenocarcinoma: Retrospective study and review of the literature.World J Gastroenterol. 2017 Sep 21;23(35):6420-6428. doi: 10.3748/wjg.v23.i35.6420. World J Gastroenterol. 2017. PMID: 29085191 Free PMC article. Review.
-
The role of pulmonary metastasectomy in patients suffering pancreatic ductal adenocarcinoma with lung metastases: a systematic review and meta-analysis.Front Surg. 2025 Feb 27;12:1535212. doi: 10.3389/fsurg.2025.1535212. eCollection 2025. Front Surg. 2025. PMID: 40084343 Free PMC article.
Cited by
-
Essential updates 2021/2022: Surgical outcomes of oligometastasis in pancreatic ductal adenocarcinoma.Ann Gastroenterol Surg. 2023 Jan 18;7(3):358-366. doi: 10.1002/ags3.12655. eCollection 2023 May. Ann Gastroenterol Surg. 2023. PMID: 37152775 Free PMC article. Review.
-
Surgery for Oligometastatic Pancreatic Cancer: Defining Biologic Resectability.Ann Surg Oncol. 2024 Jun;31(6):4031-4041. doi: 10.1245/s10434-024-15129-8. Epub 2024 Mar 19. Ann Surg Oncol. 2024. PMID: 38502293 Free PMC article. Review.
-
Defining oligometastatic pancreatic cancer: a systematic review and critical synthesis of consensus.ESMO Open. 2023 Dec;8(6):102067. doi: 10.1016/j.esmoop.2023.102067. Epub 2023 Nov 20. ESMO Open. 2023. PMID: 37988953 Free PMC article.
-
Long non-coding RNA LINC00930 targeting miR-6792-3p/ZBTB16 regulates the proliferation and EMT of pancreatic cancer.BMC Cancer. 2024 May 24;24(1):638. doi: 10.1186/s12885-024-12365-9. BMC Cancer. 2024. PMID: 38789960 Free PMC article.
-
Risk and prognostic factors of survival for patients with pancreatic ductal adenocarcinoma metastasis to lung: a cohort study.Front Oncol. 2025 May 21;15:1521616. doi: 10.3389/fonc.2025.1521616. eCollection 2025. Front Oncol. 2025. PMID: 40469173 Free PMC article.
References
-
- Tempero M.A., Malafa M.P., Al-Hawary M., Behrman S.W., Benson A.B., Cardin D.B., Chiorean E.G., Chung V., Czito B., Del Chiaro M., et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2021;19:439–457. doi: 10.6004/jnccn.2021.0017. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
