

Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma
- PMID: 35565248
- PMCID: PMC9104786
- DOI: 10.3390/cancers14092120
Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma
Abstract
Background: Primary sclerosing cholangitis (PSC) is a major risk factor for cholangiocarcinoma (CCA). We investigated biliary and fecal microbiota to determine whether specific microbes in the bile or stool are associated with PSC or CCA.
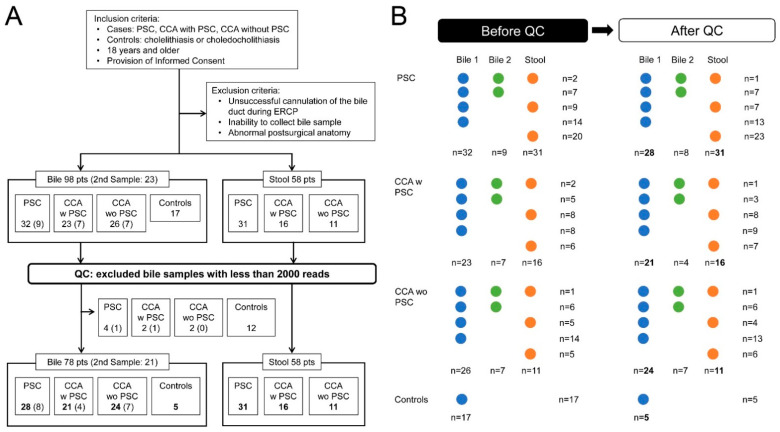
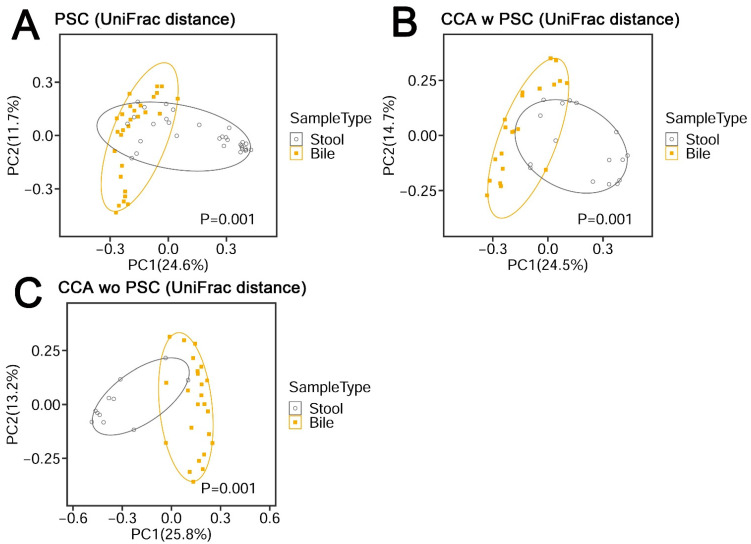
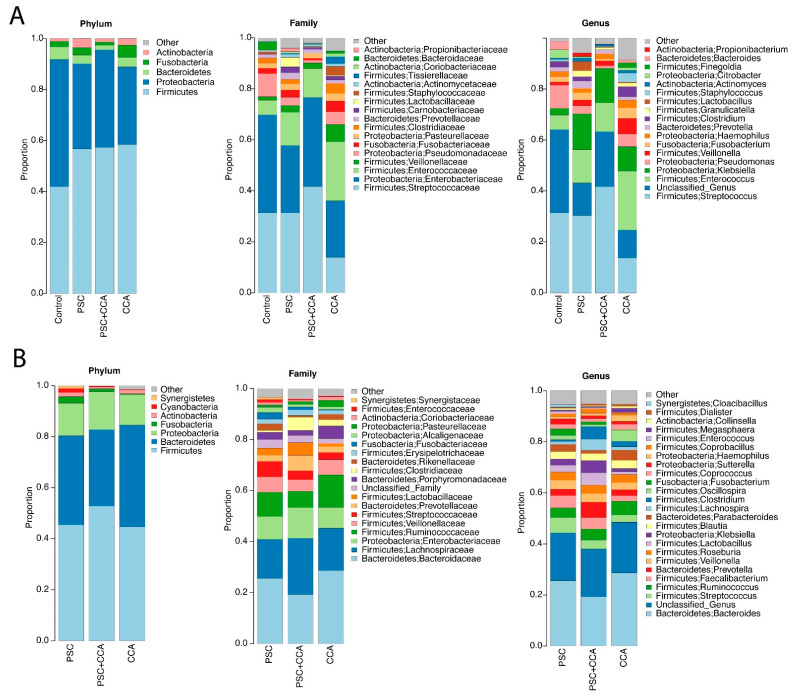
Methods: Bile was obtained from 32 patients with PSC, 23 with CCA with PSC, 26 with CCA without PSC, and 17 controls. Over 90% of bile samples were from patients with perihilar CCA. Stool was obtained from 31 patients with PSC (11 were matched to bile), 16 with CCA with PSC (10 matched to bile), and 11 with CCA without PSC (6 matched to bile). Microbiota composition was assessed using 16SrRNA-marker-based sequencing and was compared between groups.
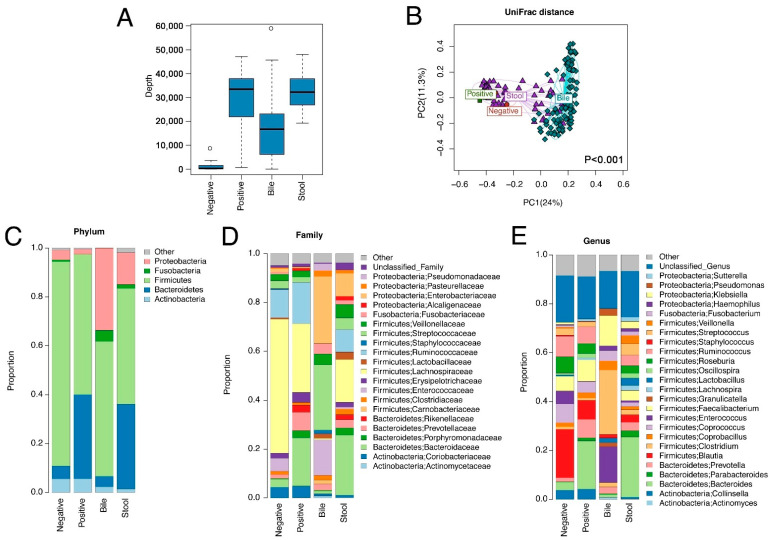
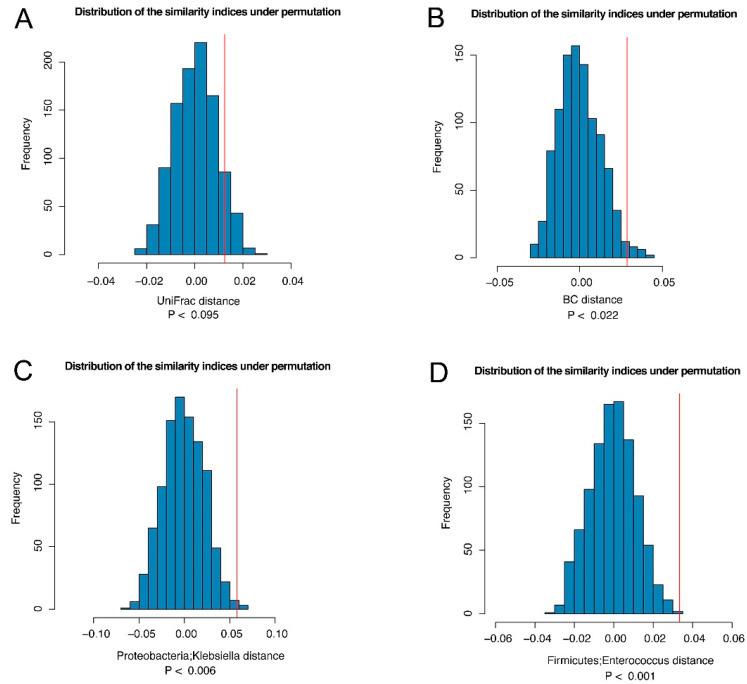
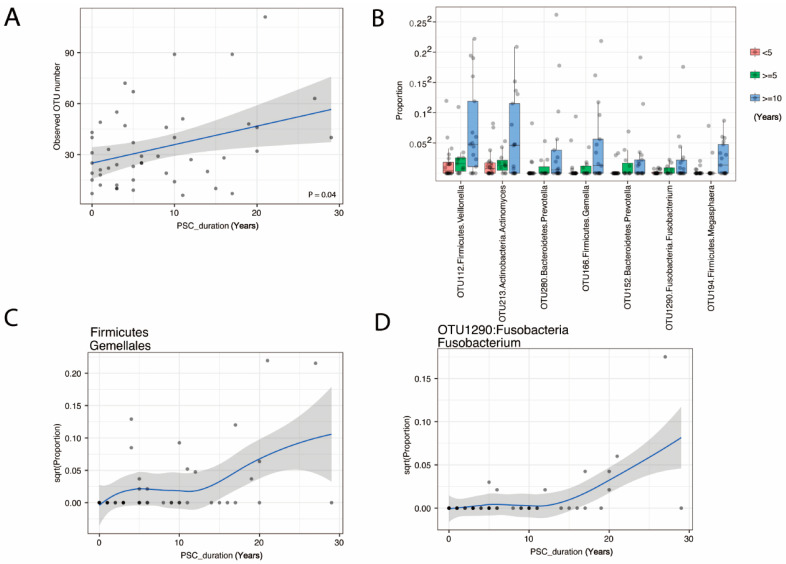
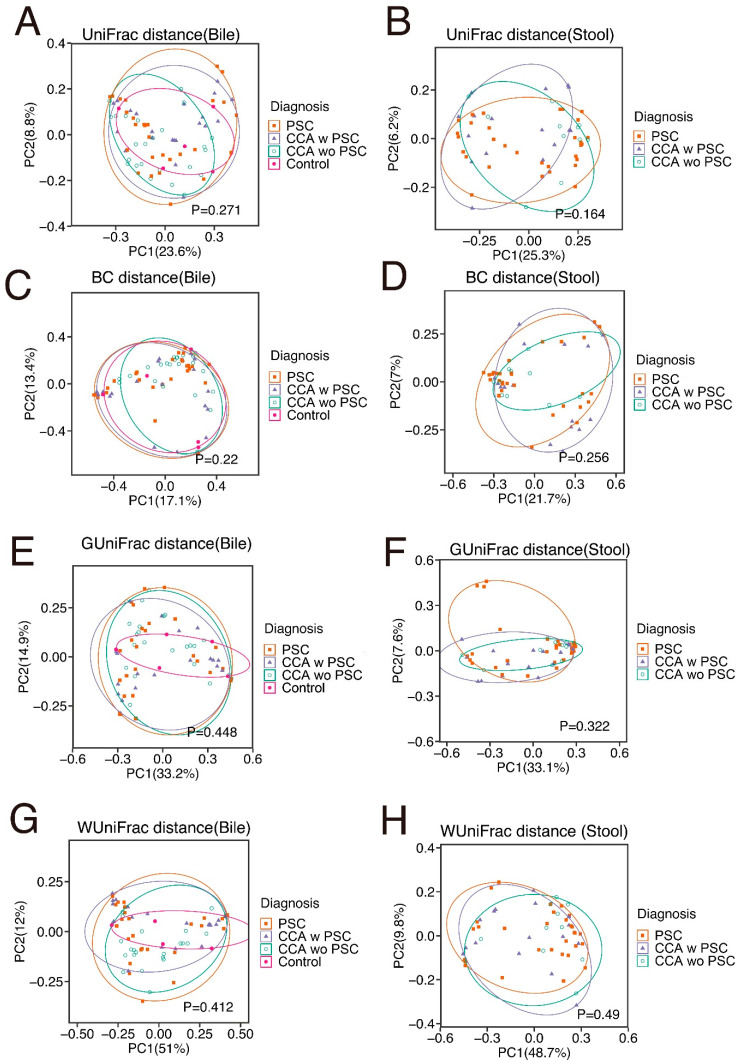
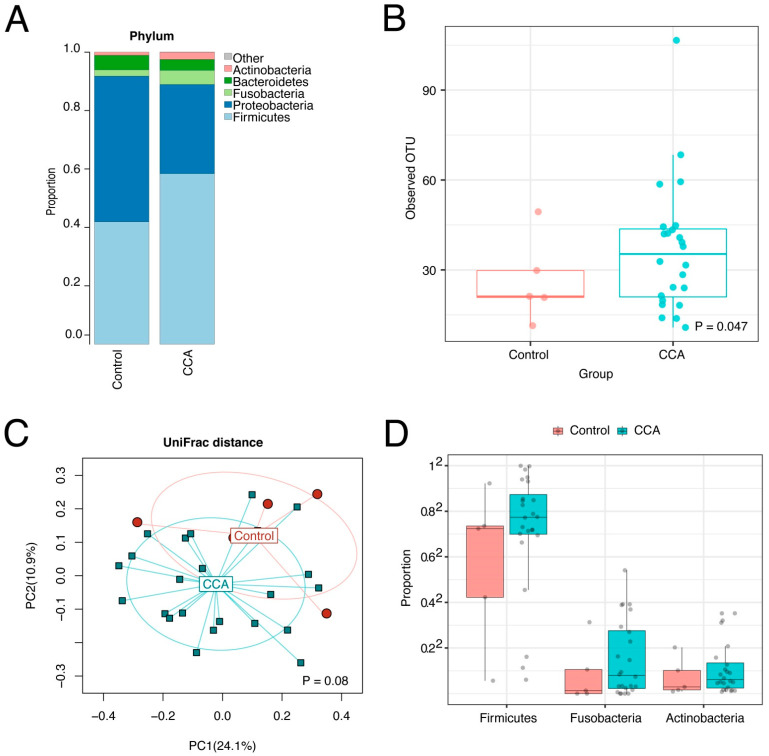
Results: Bile has a unique microbiota distinguished from negative DNA controls and stool. Increased species richness and abundance of Fusobacteria correlated with duration of PSC and characterized the biliary microbiota in CCA. Stool microbiota composition showed no significant differences between groups.
Conclusions: We identified a unique microbial signature in the bile of patients with increased duration of PSC or with CCA, suggesting a role for microbiota-driven inflammation in the pathogenesis and or progression to perihilar CCA. Further studies are needed to test this hypothesis.
Keywords: bile microbiome; cholangiocarcinoma; primary sclerosing cholangitis.
Conflict of interest statement
L.R.R. has received grant funding from Bayer, Boston Scientific, Exact Sciences, Gilead Sciences, Glycotest, Redhill Biopharma, TARGET PharmaSolutions, and FUJIFILM Medical Systems and has served on advisory boards for AstraZeneca, Bayer, Eisai, Exact Sciences, Gilead Sciences, and QED Therapeutics.
Figures
References
-
- Banales J.M., Marin J.J.G., Lamarca A., Rodrigues P.M., Khan S.A., Roberts L.R., Cardinale V., Carpino G., Andersen J.B., Braconi C., et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020;17:557–588. doi: 10.1038/s41575-020-0310-z. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
