

Spatial Characterization of Tumor-Infiltrating Lymphocytes and Breast Cancer Progression
- PMID: 35565277
- PMCID: PMC9105398
- DOI: 10.3390/cancers14092148
Spatial Characterization of Tumor-Infiltrating Lymphocytes and Breast Cancer Progression
Abstract
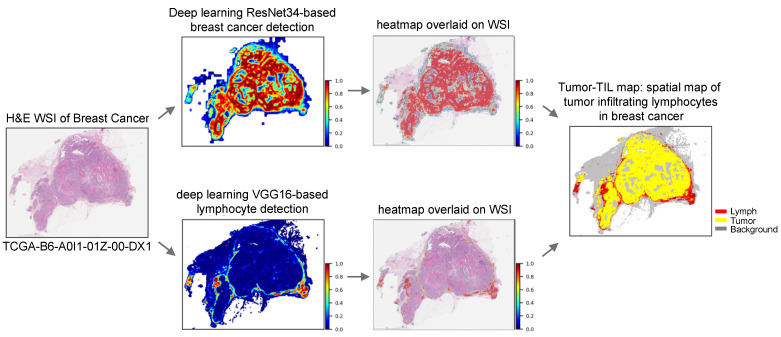
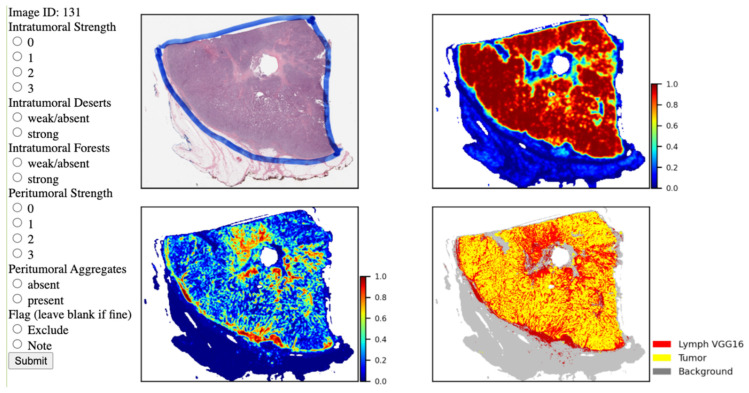
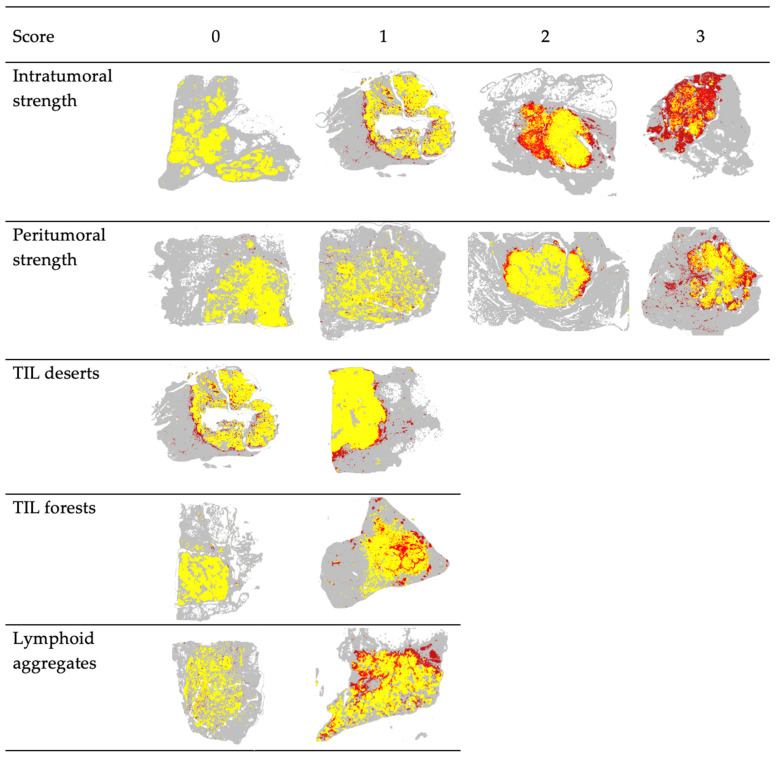
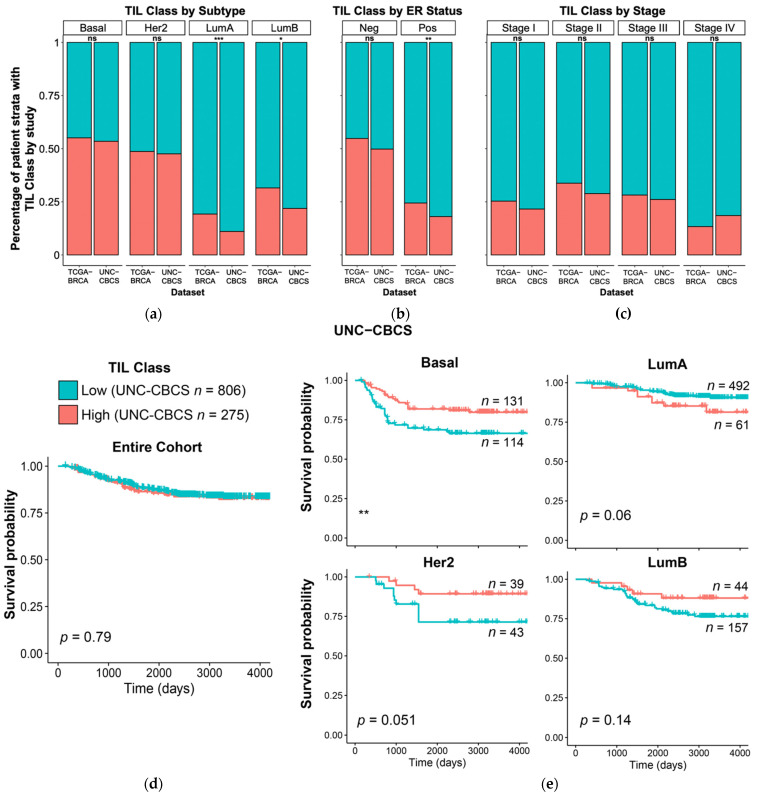
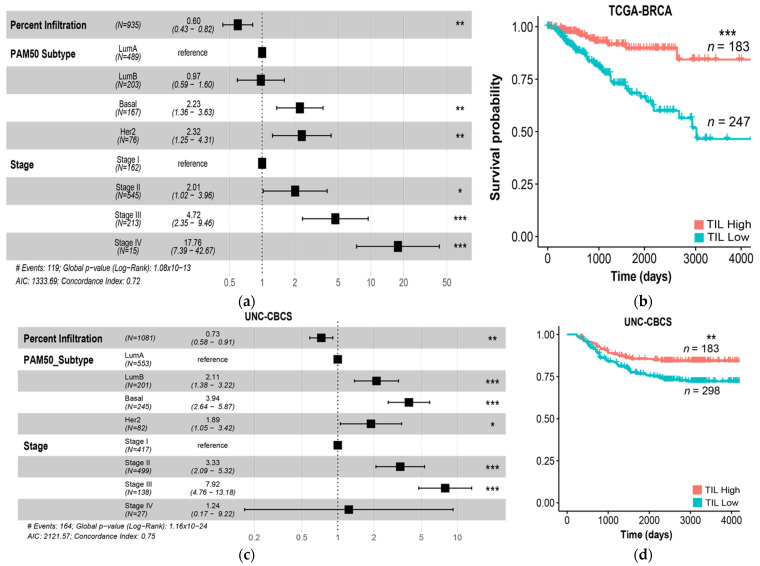
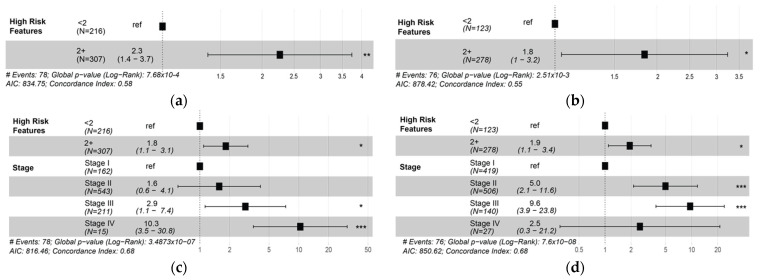
Tumor-infiltrating lymphocytes (TILs) have been established as a robust prognostic biomarker in breast cancer, with emerging utility in predicting treatment response in the adjuvant and neoadjuvant settings. In this study, the role of TILs in predicting overall survival and progression-free interval was evaluated in two independent cohorts of breast cancer from the Cancer Genome Atlas (TCGA BRCA) and the Carolina Breast Cancer Study (UNC CBCS). We utilized machine learning and computer vision algorithms to characterize TIL infiltrates in digital whole-slide images (WSIs) of breast cancer stained with hematoxylin and eosin (H&E). Multiple parameters were used to characterize the global abundance and spatial features of TIL infiltrates. Univariate and multivariate analyses show that large aggregates of peritumoral and intratumoral TILs (forests) were associated with longer survival, whereas the absence of intratumoral TILs (deserts) is associated with increased risk of recurrence. Patients with two or more high-risk spatial features were associated with significantly shorter progression-free interval (PFI). This study demonstrates the practical utility of Pathomics in evaluating the clinical significance of the abundance and spatial patterns of distribution of TIL infiltrates as important biomarkers in breast cancer.
Keywords: TILs; breast cancer; computational pathology; machine learning; risk of recurrence.
Conflict of interest statement
The University of North Carolina, Chapel Hill has a license of intellectual property interest in GeneCentric Diagnostics and BioClassifier, LLC, which may be used in this study. The University of North Carolina, Chapel Hill may benefit from this interest that is/are related to this research. The terms of this arrangement have been reviewed and approved by the University of North Carolina, Chapel Hill Conflict of Interest Program in accordance with its conflict-of-interest policies.
Figures
References
-
- Virchow R. Die krankhaften Geschwülste; Dreissig Vorlesungen: Gehalten Während des Wintersemesters. Volume 2. Universität zu Berlin; Berlin, Germany: 1862. p. 1865.
-
- Ehrlich P. Experimentelle Studien an Mausetumoren. Z Krebsforsch. 1907;5:59–81. doi: 10.1007/BF02015526. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
