

Vulvar Cancer: 2021 Revised FIGO Staging System and the Role of Imaging
- PMID: 35565394
- PMCID: PMC9102312
- DOI: 10.3390/cancers14092264
Vulvar Cancer: 2021 Revised FIGO Staging System and the Role of Imaging
Abstract
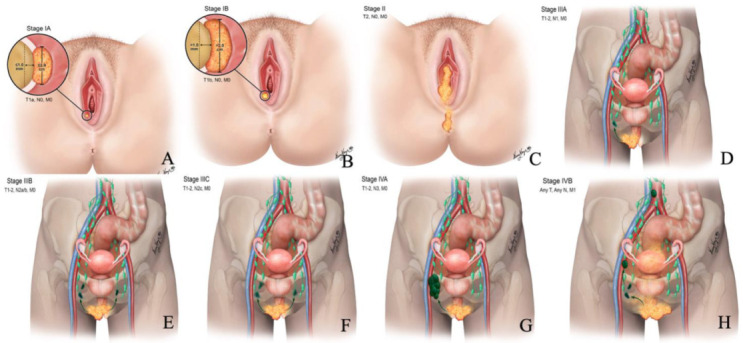
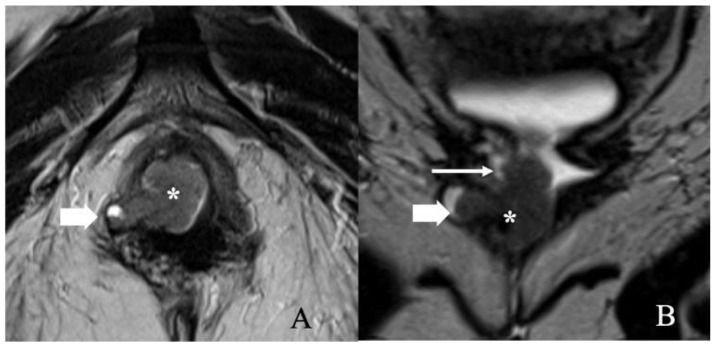
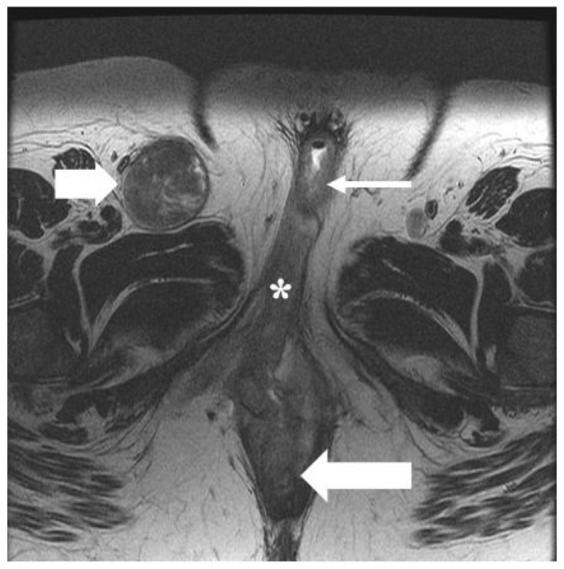
Vulvar cancer is a rare gynecological malignancy. It constitutes 5-8% of all gynecologic neoplasms, and squamous cell carcinoma is the most common variant. This article aims to review the etiopathogenesis revised 2021 International Federation of Gynecology and Obstetrics (FIGO) classification and emphasize imaging in the staging of vulvar cancer. The staging has been regulated by FIGO since 1969 and is subjected to multiple revisions. Previous 2009 FIGO classification is limited by the prognostic capability, which prompted the 2021 revisions and issue of a new FIGO classification. Although vulvar cancer can be visualized clinically, imaging plays a crucial role in the staging of the tumor, assessing the tumor extent, and planning the management. In addition, sentinel lymph node biopsy facilitates the histopathological staging of the draining lymph node, thus enabling early detection of tumor metastases and better survival rates.
Keywords: 2021 vulvar cancer staging; FIGO staging; imaging of vulvar cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures








Similar articles
-
A prognostic nomogram based on lymph node ratio for postoperative vulvar squamous cell carcinoma from the Surveillance, Epidemiology, and End Results database: a retrospective cohort study.Ann Transl Med. 2020 Nov;8(21):1382. doi: 10.21037/atm-20-3240. Ann Transl Med. 2020. PMID: 33313127 Free PMC article.
-
Gynecologic tumor board: a radiologist's guide to vulvar and vaginal malignancies.Abdom Radiol (NY). 2021 Dec;46(12):5669-5686. doi: 10.1007/s00261-021-03209-2. Epub 2021 Aug 25. Abdom Radiol (NY). 2021. PMID: 34435227 Free PMC article. Review.
-
Multimodality imaging of vulvar cancer: staging, therapeutic response, and complications.AJR Am J Roentgenol. 2013 Jun;200(6):1387-400. doi: 10.2214/AJR.12.9714. AJR Am J Roentgenol. 2013. PMID: 23701080 Review.
-
Clinical significance and prognostic value of femoral lymph node metastasis in FIGO stage III vulvar carcinoma.Eur J Surg Oncol. 2017 Sep;43(9):1768-1775. doi: 10.1016/j.ejso.2017.05.019. Epub 2017 May 31. Eur J Surg Oncol. 2017. PMID: 28602173
-
Staging for vulvar cancer.Best Pract Res Clin Obstet Gynaecol. 2015 Aug;29(6):802-11. doi: 10.1016/j.bpobgyn.2015.01.004. Epub 2015 Mar 4. Best Pract Res Clin Obstet Gynaecol. 2015. PMID: 25842047 Review.
Cited by
-
Is There a Place for Brachytherapy in Vulvar Cancer? A Narrative Review.Cancers (Basel). 2023 Nov 25;15(23):5581. doi: 10.3390/cancers15235581. Cancers (Basel). 2023. PMID: 38067285 Free PMC article. Review.
-
The Role of Methylation as an Epigenetic Marker in HPV-Related Oral Lesions.J Med Virol. 2025 Jul;97(7):e70459. doi: 10.1002/jmv.70459. J Med Virol. 2025. PMID: 40556436 Free PMC article.
-
MRI in the Evaluation of Locally Advanced Vulvar Cancer Treated with Chemoradiotherapy and Vulvar Cancer Recurrence: The 2021 Revision of FIGO Classification and the Need for Multidisciplinary Management.Cancers (Basel). 2022 Aug 9;14(16):3852. doi: 10.3390/cancers14163852. Cancers (Basel). 2022. PMID: 36010846 Free PMC article. Review.
-
Safety and Feasibility of Vulvar Cancer Treatment with Electrochemotherapy.Cancers (Basel). 2023 Jun 7;15(12):3079. doi: 10.3390/cancers15123079. Cancers (Basel). 2023. PMID: 37370690 Free PMC article.
-
Prognostic Factors and Quality of Life in Vulvar Cancer Patients: 12-Year Results from a Eastern European Center.J Pers Med. 2025 Jun 22;15(7):266. doi: 10.3390/jpm15070266. J Pers Med. 2025. PMID: 40710383 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Medical
