

Circulating microRNAs in Cerebrospinal Fluid and Plasma: Sensitive Tool for Detection of Secondary CNS Involvement, Monitoring of Therapy and Prediction of CNS Relapse in Aggressive B-NHL Lymphomas
- PMID: 35565434
- PMCID: PMC9103209
- DOI: 10.3390/cancers14092305
Circulating microRNAs in Cerebrospinal Fluid and Plasma: Sensitive Tool for Detection of Secondary CNS Involvement, Monitoring of Therapy and Prediction of CNS Relapse in Aggressive B-NHL Lymphomas
Abstract
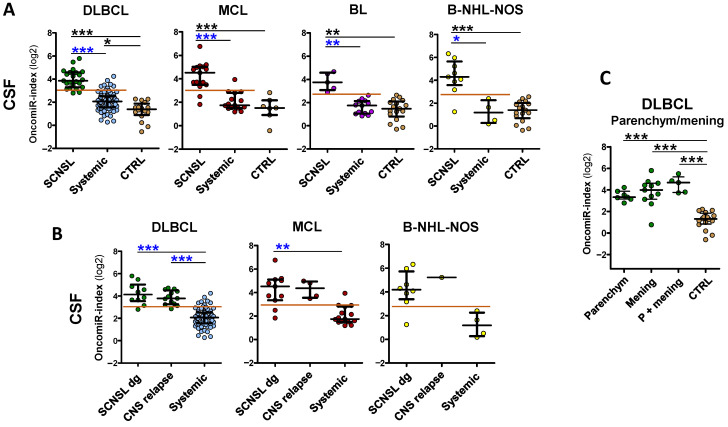
Lymphoma with secondary central nervous system (CNS) involvement represents one of the most aggressive malignancies, with poor prognosis and high mortality. New diagnostic tools for its early detection, response evaluation, and CNS relapse prediction are needed. We analyzed circulating microRNAs in the cerebrospinal fluid (CSF) and plasma of 162 patients with aggressive B-cell non-Hodgkin's lymphomas (B-NHL) and compared their levels in CNS-involving lymphomas versus in systemic lymphomas, at diagnosis and during treatment and CNS relapse. We identified a set of five oncogenic microRNAs (miR-19a, miR-20a, miR-21, miR-92a, and miR-155) in CSF that detect, with high sensitivity, secondary CNS lymphoma involvement in aggressive B-NHL, including DLBCL, MCL, and Burkitt lymphoma. Their combination into an oncomiR index enables the separation of CNS lymphomas from systemic lymphomas or nonmalignant controls with high sensitivity and specificity, and high Receiver Operating Characteristics (DLBCL AUC = 0.96, MCL = 0.93, BL = 1.0). Longitudinal analysis showed that oncomiR levels reflect treatment efficacy and clinical outcomes, allowing their monitoring and prediction. In contrast to conventional methods, CSF oncomiRs enable detection of early and residual CNS involvement, as well as parenchymal involvement. These circulating oncomiRs increase 1-4 months before CNS relapse, allowing its early detection and improving the prediction of CNS relapse risk in DLBCL. Similar effects were detectable, to a lesser extent, in plasma.
Keywords: B-NHL; Burkitt; CNS; DLBCL; MCL; cerebrospinal fluid; lymphoma; microRNA; plasma; relapse.
Conflict of interest statement
M.T. has received honoraria and research funding, and has acted as a consultant or advisor to F. Hoffmann-La Roche Ltd. The remaining authors declare no competing financial interests.
Figures





Similar articles
-
Characteristics of Central Nervous System (CNS) Involvement in Children With Non-Hodgkin's Lymphoma (NHL) and the Diagnostic Value of CSF Flow Cytometry in CNS Positive Disease.Technol Cancer Res Treat. 2021 Jan-Dec;20:15330338211016372. doi: 10.1177/15330338211016372. Technol Cancer Res Treat. 2021. PMID: 34060372 Free PMC article.
-
Epstein-Barr virus DNA load in cerebrospinal fluid and plasma of patients with AIDS-related lymphoma.J Neurovirol. 2002 Oct;8(5):432-8. doi: 10.1080/13550280260422730. J Neurovirol. 2002. PMID: 12402169
-
A Set of 17 microRNAs Common for Brain and Cerebrospinal Fluid Differentiates Primary Central Nervous System Lymphoma from Non-Malignant Brain Tumors.Biomolecules. 2021 Sep 21;11(9):1395. doi: 10.3390/biom11091395. Biomolecules. 2021. PMID: 34572608 Free PMC article.
-
Rituximab: a review of its use in non-Hodgkin's lymphoma and chronic lymphocytic leukaemia.Drugs. 2003;63(8):803-43. doi: 10.2165/00003495-200363080-00005. Drugs. 2003. PMID: 12662126 Review.
-
Modern cerebrospinal fluid analyses for the diagnosis of diffuse large B-cell lymphoma of the CNS.CNS Oncol. 2014 Jan;3(1):77-85. doi: 10.2217/cns.13.63. CNS Oncol. 2014. PMID: 25054902 Free PMC article. Review.
Cited by
-
Liquid biopsy for improving diagnosis and monitoring of CNS lymphomas: A RANO review.Neuro Oncol. 2024 Jun 3;26(6):993-1011. doi: 10.1093/neuonc/noae032. Neuro Oncol. 2024. PMID: 38598668 Free PMC article. Review.
-
Prognostic Value of the miR-17~92 Cluster in Chronic Lymphocytic Leukemia.Int J Mol Sci. 2023 Jan 15;24(2):1705. doi: 10.3390/ijms24021705. Int J Mol Sci. 2023. PMID: 36675221 Free PMC article.
-
Outcome of patients with diffuse large B-cell lymphoma and testicular involvement - real world data.Ann Hematol. 2025 Jan;104(1):675-684. doi: 10.1007/s00277-024-06025-y. Epub 2024 Oct 1. Ann Hematol. 2025. PMID: 39352469 Free PMC article.
-
Diffuse large B-cell lymphoma with contemporary involvement of central and peripheral nervous system: A case report and literature review.Heliyon. 2024 Mar 21;10(7):e28552. doi: 10.1016/j.heliyon.2024.e28552. eCollection 2024 Apr 15. Heliyon. 2024. PMID: 38560176 Free PMC article.
References
-
- El-Galaly T.C., Cheah C.Y., Bendtsen M.D., Nowakowski G.S., Kansara R., Savage K.J., Connors J.M., Sehn L.H., Goldschmidt N., Shaulov A., et al. Treatment strategies, outcomes and prognostic factors in 291 patients with secondary CNS involvement by diffuse large B-cell lymphoma. Eur. J. Cancer. 2018;93:57–68. doi: 10.1016/j.ejca.2018.01.073. - DOI - PMC - PubMed
-
- Cheah C.Y., George A., Gine E., Chiappella A., Kluin-Nelemans H.C., Jurczak W., Krawczyk K., Mocikova H., Klener P., Salek D., et al. Central nervous system involvement in mantle cell lymphoma: Clinical features, prognostic factors and outcomes from the European Mantle Cell Lymphoma Network. Ann. Oncol. 2013;24:2119–2123. doi: 10.1093/annonc/mdt139. - DOI - PubMed
LinkOut - more resources
Full Text Sources
