

Phase Angle Is a Stronger Predictor of Hospital Outcome than Subjective Global Assessment-Results from the Prospective Dessau Hospital Malnutrition Study
- PMID: 35565747
- PMCID: PMC9100773
- DOI: 10.3390/nu14091780
Phase Angle Is a Stronger Predictor of Hospital Outcome than Subjective Global Assessment-Results from the Prospective Dessau Hospital Malnutrition Study
Abstract
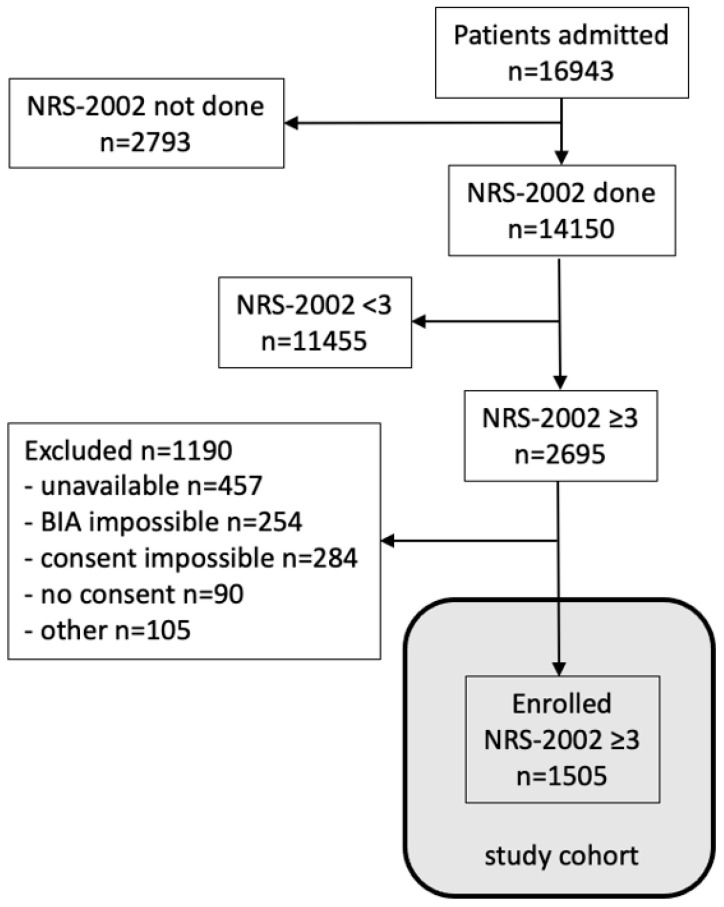
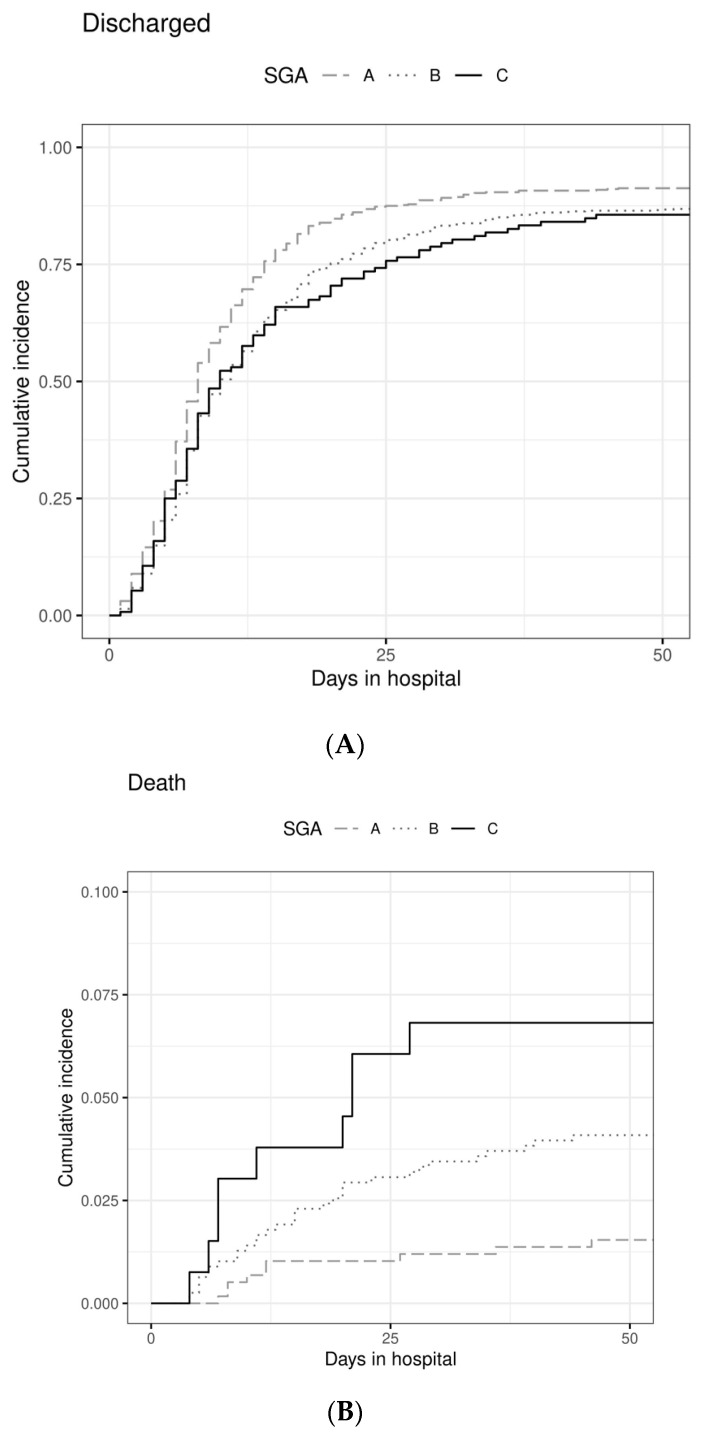
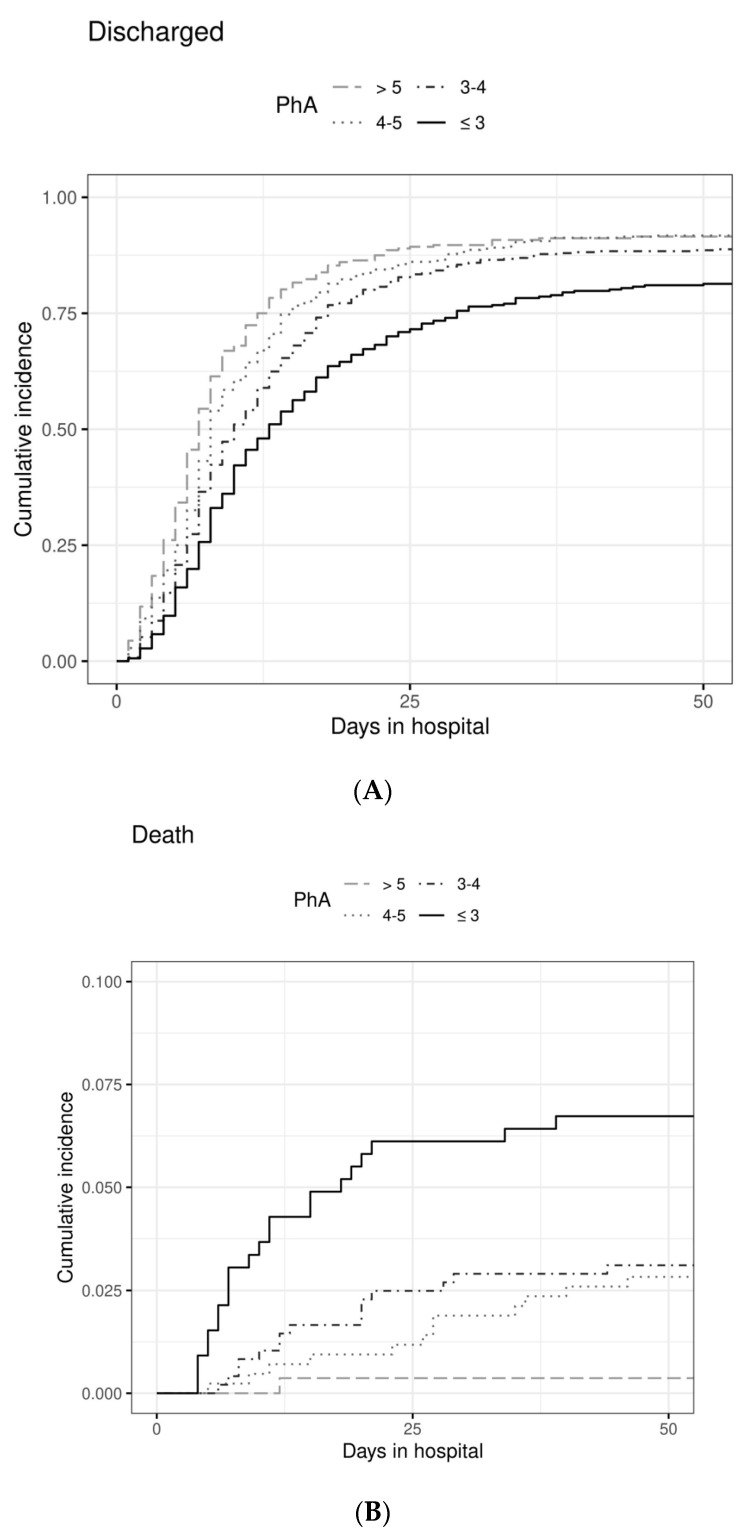
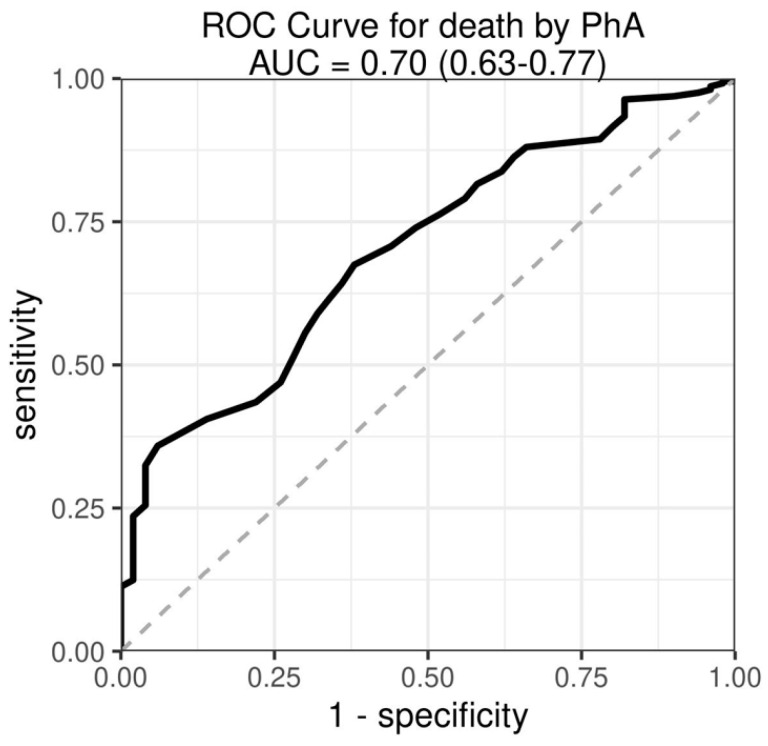
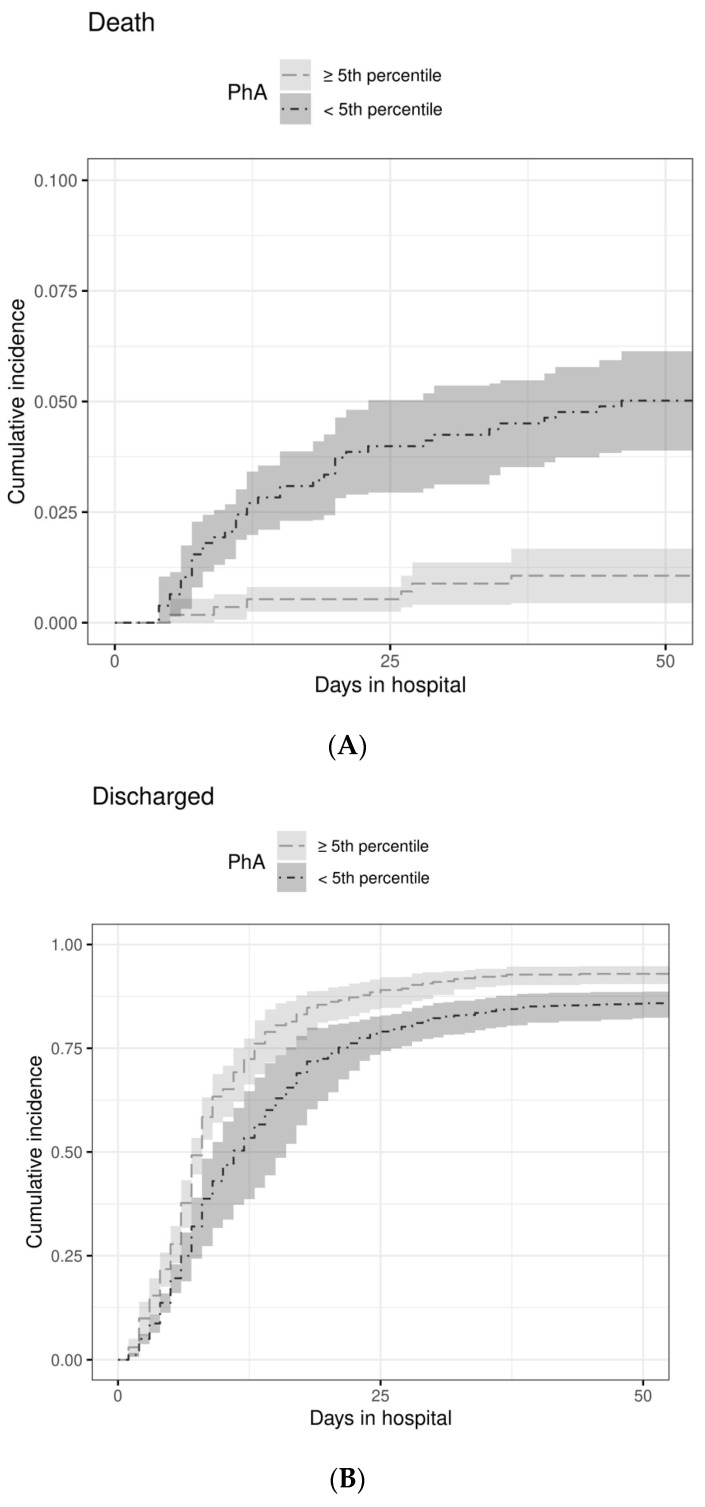
This prospective cohort study of 16,943 consecutive patients compared phase angle (PhA, foot-to-hand at 50 kHz) and subjective global assessment (SGA) to predict outcomes length of hospital stay (LOS) and in-hospital mortality in patients at risk of malnutrition (NRS-2002 ≥ 3). In 1505 patients, the independent effects on LOS were determined by competing risk analysis and on mortality by logistic regression. In model I, including influence factors age, sex, BMI, and diagnoses, malnourished (SGA B and C) patients had a lower chance for a regular discharge (HR 0.74; 95%CI 0.69−0.79) and an increased risk of mortality (OR 2.87; 95%CI 1.38−5.94). The association of SGA and outcomes regular discharge and mortality was completely abrogated when PhA was added (model II). Low PhA reduced the chance of a regular discharge by 53% in patients with a PhA ≤ 3° (HR 0.47; 95%CI 0.39−0.56) as compared to PhA > 5°. Mortality was reduced by 56% for each 1° of PhA (OR 0.44; 95%CI 0.32−0.61). Even when CRP was added in model III, PhA ≤ 3° was associated with a 41% lower chance for a regular discharge (HR 0.59; 95%CI 0.48−0.72). In patients at risk of malnutrition, the objective measure PhA was a stronger predictor of LOS and mortality than SGA.
Keywords: bioimpedance analysis; inflammatory status; medical patients; nutritional status; screening; surgical patients.
Conflict of interest statement
M.P. has received speaker’s honoraria from Fresenius Kabi. M.H. has received speaker’s honoraria from Fresenius Kabi and Nutricia and unrestricted grants to Medical University of Vienna from Abbott, Baxter, Fresenius.
Figures
Similar articles
-
Low phase angle determined by bioelectrical impedance analysis is associated with malnutrition and nutritional risk at hospital admission.Clin Nutr. 2013 Apr;32(2):294-9. doi: 10.1016/j.clnu.2012.08.001. Epub 2012 Aug 14. Clin Nutr. 2013. PMID: 22921419
-
Usefulness of six diagnostic and screening measures for undernutrition in predicting length of hospital stay: a comparative analysis.J Acad Nutr Diet. 2015 Jun;115(6):927-38. doi: 10.1016/j.jand.2014.11.015. Epub 2015 Jan 27. J Acad Nutr Diet. 2015. PMID: 25634094
-
Nutritional assessment: comparison of clinical assessment and objective variables for the prediction of length of hospital stay and readmission.Am J Clin Nutr. 2015 May;101(5):956-65. doi: 10.3945/ajcn.114.098665. Epub 2015 Mar 4. Am J Clin Nutr. 2015. PMID: 25739926
-
Phase Angle and Handgrip Strength as a Predictor of Disease-Related Malnutrition in Admitted Patients: 12-Month Mortality.Nutrients. 2022 Apr 28;14(9):1851. doi: 10.3390/nu14091851. Nutrients. 2022. PMID: 35565818 Free PMC article.
-
Decline in nutritional status is associated with prolonged length of stay in hospitalized patients admitted for 7 days or more: A prospective cohort study.Clin Nutr. 2016 Feb;35(1):144-152. doi: 10.1016/j.clnu.2015.01.009. Epub 2015 Jan 21. Clin Nutr. 2016. PMID: 25660316
Cited by
-
[Sarcopenia in chronic liver diseases].Inn Med (Heidelb). 2023 Jun;64(6):525-531. doi: 10.1007/s00108-023-01526-w. Epub 2023 May 23. Inn Med (Heidelb). 2023. PMID: 37219562 Review. German.
-
Role of phase angle in older adults with focus on the geriatric syndromes sarcopenia and frailty.Rev Endocr Metab Disord. 2023 Jun;24(3):429-437. doi: 10.1007/s11154-022-09772-3. Epub 2022 Dec 2. Rev Endocr Metab Disord. 2023. PMID: 36456777 Free PMC article. Review.
-
Phase Angle Predicts Malnutrition Risk and 6-month Mortality in Older Patients with Multimorbidity: A Retrospective Study.Clin Interv Aging. 2025 Jun 26;20:895-902. doi: 10.2147/CIA.S518795. eCollection 2025. Clin Interv Aging. 2025. PMID: 40599689 Free PMC article.
-
Predicting the unseen: nutritional interventions as a key to combat frailty.Front Nutr. 2025 Jul 9;12:1575922. doi: 10.3389/fnut.2025.1575922. eCollection 2025. Front Nutr. 2025. PMID: 40704314 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
