

Vitamin D in Osteosarcopenic Obesity
- PMID: 35565781
- PMCID: PMC9100750
- DOI: 10.3390/nu14091816
Vitamin D in Osteosarcopenic Obesity
Abstract
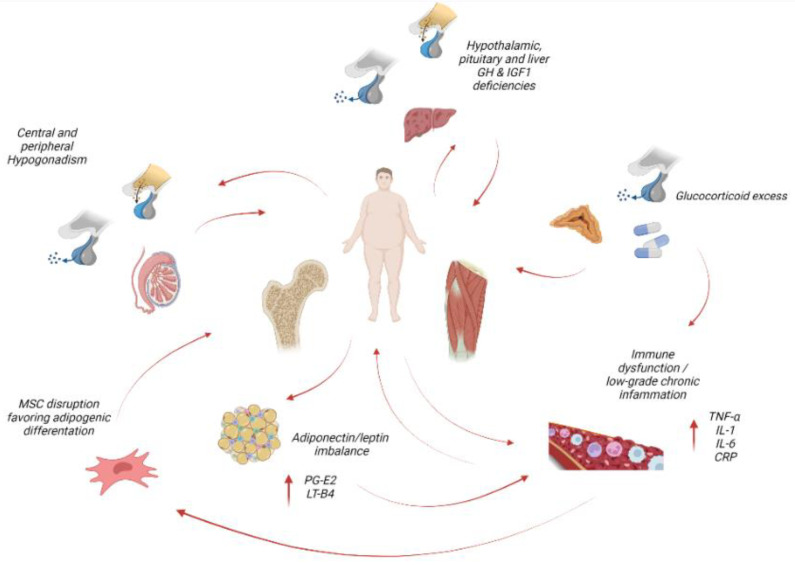
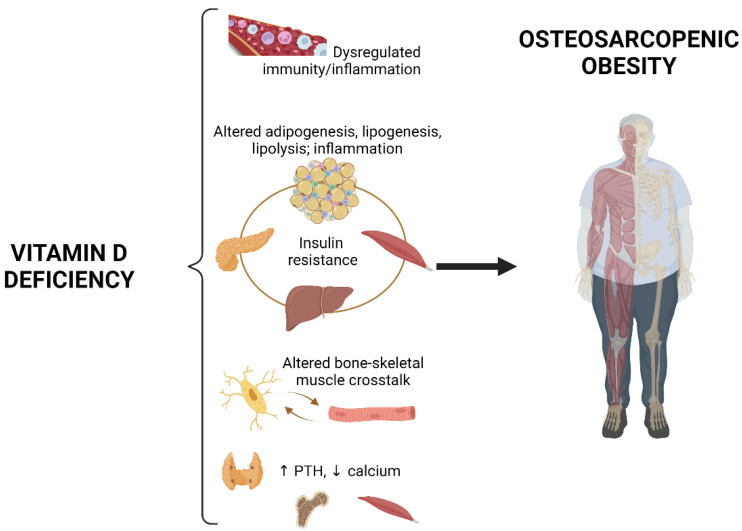
Osteosarcopenic obesity is a unique clinical condition where low bone and muscle mass coexist in individuals with obesity. Alterations in adipose tissue, skeletal muscle and bone are strictly interconnected, and vitamin D plays key roles in several metabolic pathways that are involved in maintaining musculoskeletal health and glucose homeostasis. We reviewed the available literature on mechanisms underlying osteosarcopenic obesity, with a focus on the role of vitamin D in the pathogenesis and treatment of the condition. We found that, although evidence from large observational studies and pre-clinical experiments strongly supports a role of vitamin D deficiency in the pathogenesis of osteosarcopenic obesity, the common belief that vitamin D improves musculoskeletal health lacks solid clinical evidence, as trials specifically aimed at assessing the effects of vitamin D supplementation in patients with osteosarcopenic obesity are not available, and trials that investigated the role of vitamin D on muscle and bone health in other patient populations either showed no or even detrimental effects. We conclude that large observational and interventional studies including individuals with osteosarcopenic obesity representative of different sex, age and race are needed to better define the role of vitamin D in the pathogenesis and treatment of this condition.
Keywords: insulin resistance; obesity; osteopenia; osteoporosis; sarcopenia; sarcopenic obesity; vitamin D.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Donini L.M., Busetto L., Bischoff S.C., Cederholm T., Ballesteros-Pomar M.D., Batsis J.A., Bauer J.M., Boirie Y., Cruz-Jentoft A.J., Dicker D., et al. Definition and diagnostic criteria for sarcopenic obesity: ESPEN and EASO consensus statement. Clin. Nutr. 2022;41:990–1000. doi: 10.1016/j.clnu.2021.11.014. - DOI - PubMed
-
- Turcotte A.F., O’Connor S., Morin S.N., Gibbs J.C., Willie B.M., Jean S., Gagnon C. Association between obesity and risk of fracture, bone mineral density and bone quality in adults: A systematic review and meta-analysis. PLoS ONE. 2021;16:e0252487. doi: 10.1371/journal.pone.0252487. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
