

Carbohydrate Maldigestion and Intolerance
- PMID: 35565890
- PMCID: PMC9099680
- DOI: 10.3390/nu14091923
Carbohydrate Maldigestion and Intolerance
Abstract
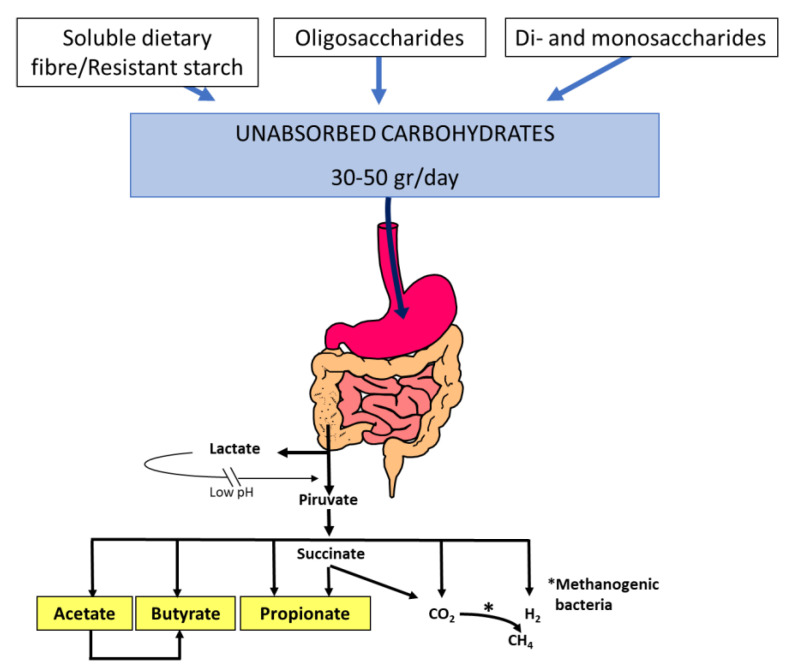
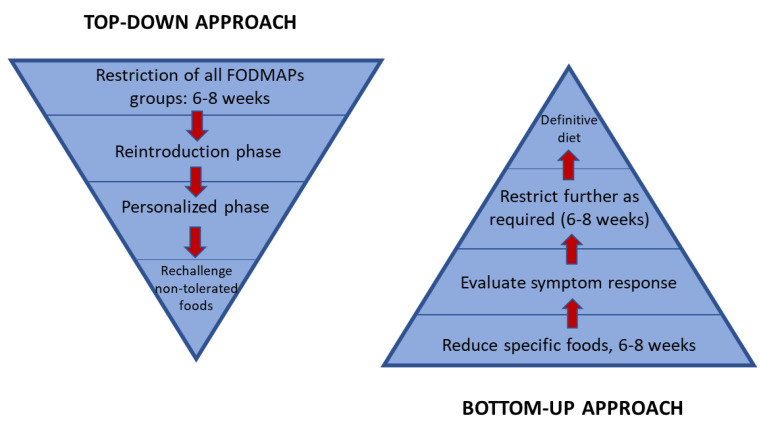
This review summarizes dietary carbohydrate intolerance conditions and recent advances on the possible role of carbohydrate maldigestion and dietary outcomes in patients with functional bowel disease. When malabsorbed carbohydrates reach the colon, they are fermented by colonic bacteria, with the production of short-chain fatty acids and gas lowering colonic pH. The appearance of diarrhoea or symptoms of flatulence depends in part on the balance between the production and elimination of these fermentation products. Different studies have shown that there are no differences in the frequency of sugar malabsorption between patients with irritable bowel disease (IBS) and healthy controls; however, the severity of symptoms after a sugar challenge is higher in patients than in controls. A diet low in 'Fermentable, Oligo-Di- and Monosaccharides and Polyols' (FODMAPs) is an effective treatment for global symptoms and abdominal pain in IBS, but its implementation should be supervised by a trained dietitian. A 'bottom-up' approach to the low-FODMAP diet has been suggested to avoid an alteration of gut microbiota and nutritional status. Two approaches have been suggested in this regard: starting with only certain subgroups of the low-FODMAP diet based on dietary history or with a gluten-free diet.
Keywords: FODMAP; fructose; hydrogen breath test; irritable bowel syndrome; lactose; sorbitol; sucrose; sugar malabsorption.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
