

Vitamin C and Omega-3 Fatty Acid Intake Is Associated with Human Periodontitis-A Nested Case-Control Study
- PMID: 35565905
- PMCID: PMC9101799
- DOI: 10.3390/nu14091939
Vitamin C and Omega-3 Fatty Acid Intake Is Associated with Human Periodontitis-A Nested Case-Control Study
Abstract
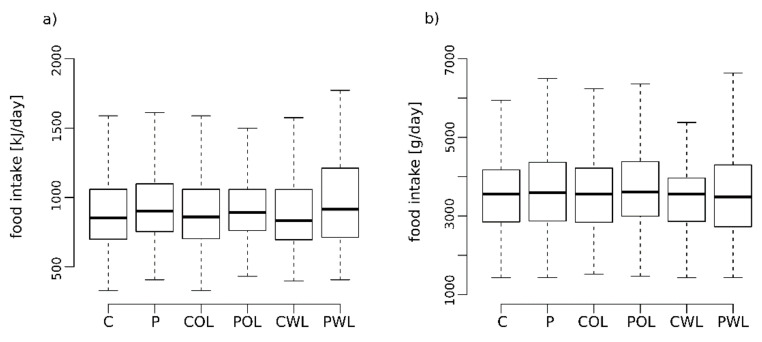
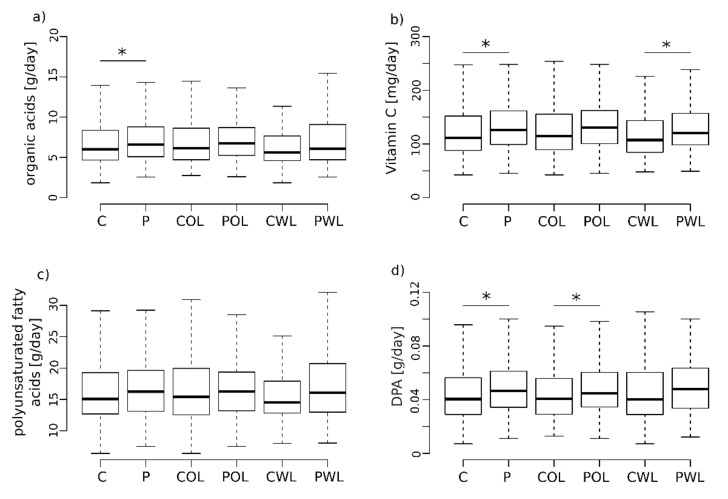
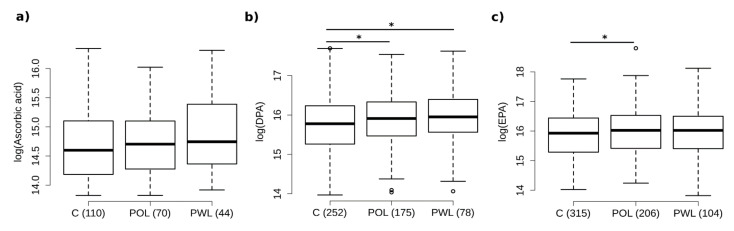
Vitamins and omega-3 fatty acids (Ω3FA) modulate periodontitis-associated inflammatory processes. The aim of the current investigation was to evaluate associations of oral nutrient intake and corresponding serum metabolites with clinical severity of human periodontitis. Within the Food Chain Plus cohort, 373 periodontitis patients—245 without (POL) and 128 with tooth loss (PWL)—were matched to 373 controls based on sex, smoking habit, age and body mass index in a nested case-control design. The amount of oral intake of vitamins and Ω3FAs was assessed from nutritional data using a Food Frequency Questionnaire. Oral intake and circulatory bioavailability of vitamins and Ω3FA serum metabolomics were compared, using ultra-high-resolution mass spectrometry. Periodontitis patients exhibited a significantly higher oral intake of vitamin C and Ω3FA Docosapentaenoic acid (p < 0.05) compared to controls. Nutritional intake of vitamin C was higher in PWL, while the intake of Docosapentaenoic acid was increased in POL (p < 0.05) compared to controls. In accordance, serum levels of Docosapentaenoic acid were also increased in POL (p < 0.01) compared to controls. Vitamin C and the Ω3FA Docosapentaenoic acid might play a role in the pathophysiology of human periodontitis. Further studies on individualized nutritional intake and periodontitis progression and therapy are necessary.
Keywords: metabolite; nutrition; omega-3 fatty acid; periodontitis; vitamin C.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Jepsen S., Blanco J., Buchalla W., Carvalho J.C., Dietrich T., Dorfer C., Eaton K.A., Figuero E., Frencken J.E., Graziani F., et al. Prevention and control of dental caries and periodontal diseases at individual and population level: Consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017;44((Suppl. 18)):S85–S93. doi: 10.1111/jcpe.12687. - DOI - PubMed
-
- Sanz M., Herrera D., Kebschull M., Chapple I., Jepsen S., Beglundh T., Sculean A., Tonetti M.S., EFP Workshop Participants. Methodological Consultants Treatment of Stage I-III Periodontitis-The EFP S3 Level Clinical Practice Guideline. J. Clin. Periodontol. 2020;47:4–60. doi: 10.1111/jcpe.13290. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
