

Secondary Osteoporosis and Metabolic Bone Diseases
- PMID: 35566509
- PMCID: PMC9102221
- DOI: 10.3390/jcm11092382
Secondary Osteoporosis and Metabolic Bone Diseases
Abstract
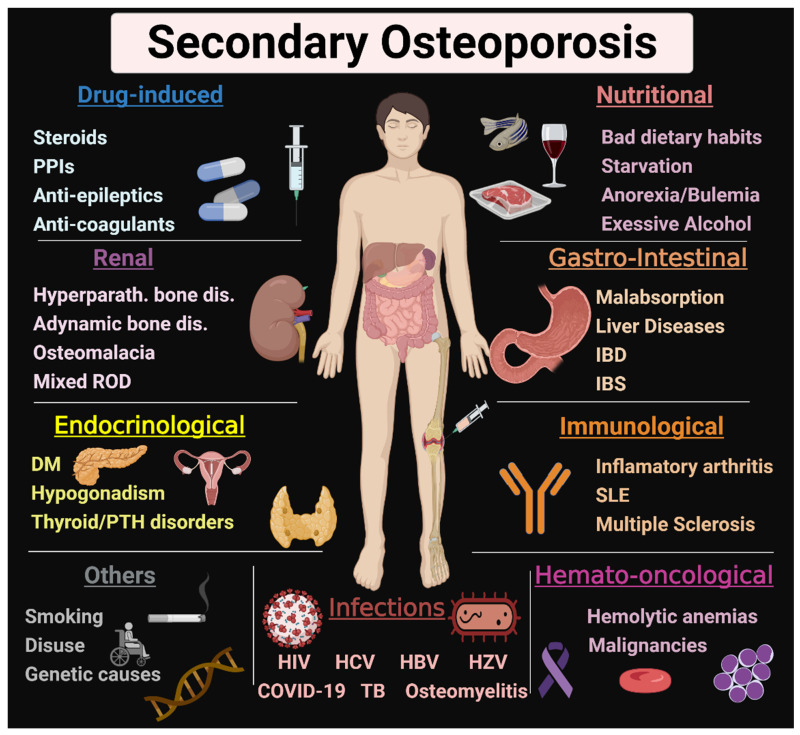
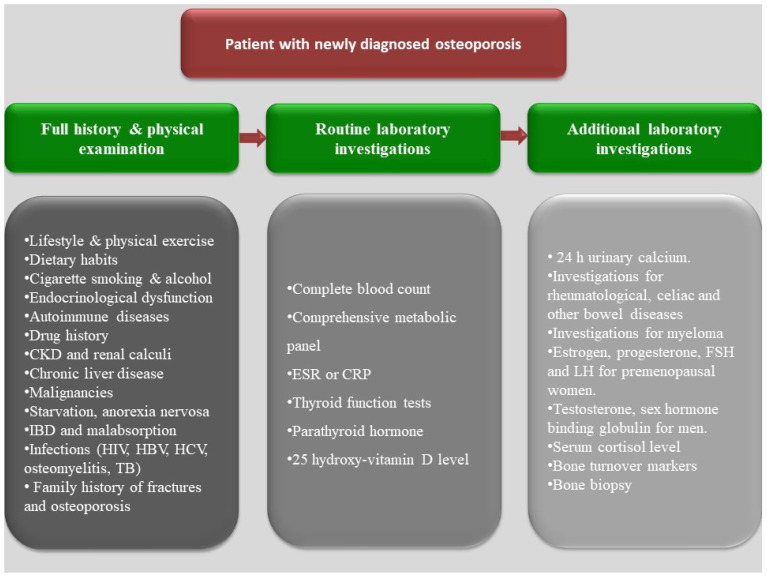
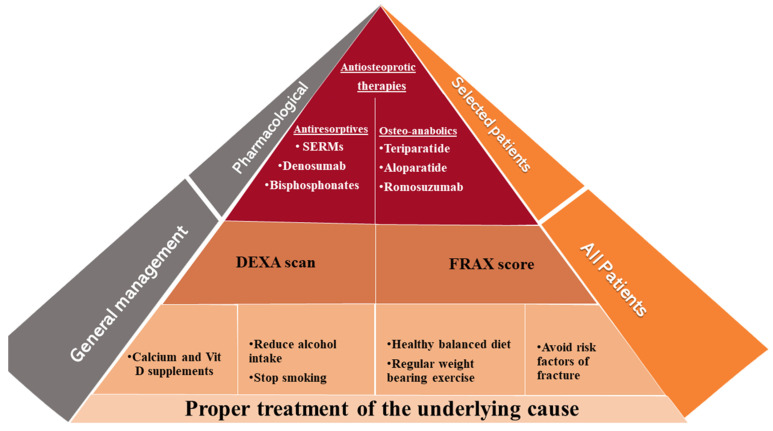
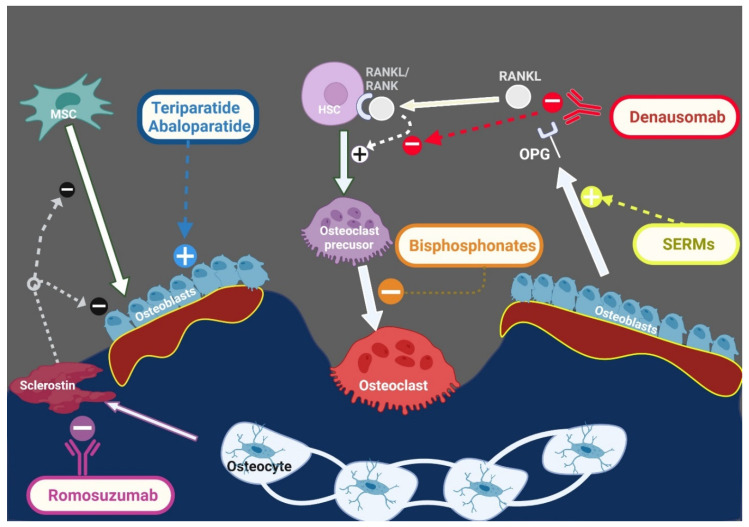
Fragility fracture is a worldwide problem and a main cause of disability and impaired quality of life. It is primarily caused by osteoporosis, characterized by impaired bone quantity and or quality. Proper diagnosis of osteoporosis is essential for prevention of fragility fractures. Osteoporosis can be primary in postmenopausal women because of estrogen deficiency. Secondary forms of osteoporosis are not uncommon in both men and women. Most systemic illnesses and organ dysfunction can lead to osteoporosis. The kidney plays a crucial role in maintaining physiological bone homeostasis by controlling minerals, electrolytes, acid-base, vitamin D and parathyroid function. Chronic kidney disease with its uremic milieu disturbs this balance, leading to renal osteodystrophy. Diabetes mellitus represents the most common secondary cause of osteoporosis. Thyroid and parathyroid disorders can dysregulate the osteoblast/osteoclast functions. Gastrointestinal disorders, malnutrition and malabsorption can result in mineral and vitamin D deficiencies and bone loss. Patients with chronic liver disease have a higher risk of fracture due to hepatic osteodystrophy. Proinflammatory cytokines in infectious, autoimmune, and hematological disorders can stimulate osteoclastogenesis, leading to osteoporosis. Moreover, drug-induced osteoporosis is not uncommon. In this review, we focus on causes, pathogenesis, and management of secondary osteoporosis.
Keywords: bone loss; bone mineral density; causes; fracture; management.
Conflict of interest statement
All the authors declared no conflict of interest in this work.
Figures
References
-
- Najar M.S., Mir M.M., Muzamil M. Prevalence of osteoporosis in patients with chronic kidney disease (stages 3–5) in comparison with age-and sex-matched controls: A study from Kashmir Valley Tertiary Care Center. Saudi J. Kidney Dis. Transpl. 2017;28:538. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
