

Methylene Blue Reduces Fluid Loading and Norepinephrine Requirements for Post-Resuscitation Syndrome in a Pig Model of Refractory Cardiac Arrest Resuscitated with Veno-Arterial ECMO
- PMID: 35566640
- PMCID: PMC9100142
- DOI: 10.3390/jcm11092515
Methylene Blue Reduces Fluid Loading and Norepinephrine Requirements for Post-Resuscitation Syndrome in a Pig Model of Refractory Cardiac Arrest Resuscitated with Veno-Arterial ECMO
Abstract
Background: Refractory cardiac arrest management relies on extracorporeal cardiopulmonary resuscitation (ECPR), requiring the use of veno-arterial extracorporeal membrane oxygenation (VA-ECMO). Circulatory flow recovery can be associated with an ischemia-reperfusion injury, leading to vasoplegia and vasopressor requirement. The aim of this work was to evaluate the impact on hemodynamics of a methylene blue bolus infusion in a porcine model of ischemic refractory cardiac arrest.
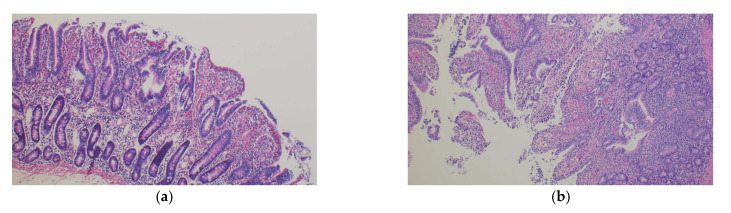
Methods: Ischemic refractory cardiac arrest was induced in 20 pigs. After a low flow period of 30 min, VA-ECMO was initiated and the pigs were randomly assigned to the standard care group (norepinephrine + crystalloids) or methylene blue group (IV 2 mg·kg-1 bolus of methylene blue over 30 min + norepinephrine and crystalloids). Macrocirculatory parameters and lactate clearance were measured. Sublingual microcirculation was evaluated with sidestream dark field (SDF) imaging. The severity of the ischemic digestive lesions was assessed according to the histologic Chiu/Park scale.
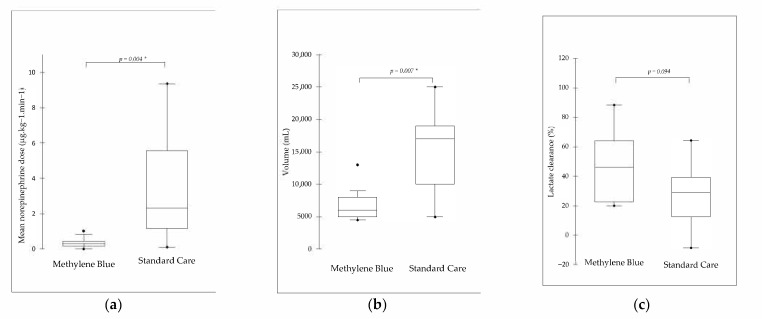
Results: Eighteen pigs were included. The total crystalloid load (5000 (6000-8000) mL vs. 17,000 (10,000-19,000) mL, p = 0.007, methylene blue vs. standard care group) and catecholamine requirements (0.31 (0.14-0.44) μg·kg-1·min-1 vs. 2.32 (1.17-5.55) μg·kg-1·min-1, methylene blue vs. standard care group, p = 0.004) were significantly reduced in the methylene blue group. There were no significant between-group differences in lactate clearance, sublingual capillary microvascular parameters assessed by SDF or histologic Chiu/Park scale.
Conclusions: In our refractory cardiac arrest porcine model treated with ECPR, methylene blue markedly reduced fluid loading and norepinephrine requirements in comparison to standard care during the first 6 h of VA-ECMO.
Keywords: advanced cardiac life support; cardiopulmonary resuscitation; extracorporeal membrane oxygenation; inflammatory response; methylene blue; microcirculation; out-of-hospital cardiac arrest; vasopressor.
Conflict of interest statement
Pr Levy received fees or grants from Abiomed, Gettinge, Orion, Amomed, Sanofi and Baxter.
Figures
References
-
- Chouihed T., Kimmoun A., Lauvray A., Laithier F.-X., Jaeger D., Lemoine S., Maureira J.P., Nace L., Duarte K., Albizzati S., et al. Improving Patient Selection for Refractory Out of Hospital Cardiac Arrest Treated with Extracorporeal Life Support. Shock. 2018;49:24–28. doi: 10.1097/SHK.0000000000000941. - DOI - PubMed
-
- Lott C., Truhlář A., Alfonzo A., Barelli A., González-Salvado V., Hinkelbein J., Nolan J.P., Paal P., Perkins G.D., Thies K.-C., et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation. 2021;161:152–219. doi: 10.1016/j.resuscitation.2021.02.011. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
