

Introducing a Pole Concept for Nodule Growth in the Thyroid Gland: Taller-than-Wide Shape, Frequency, Location and Risk of Malignancy of Thyroid Nodules in an Area with Iodine Deficiency
- PMID: 35566675
- PMCID: PMC9104008
- DOI: 10.3390/jcm11092549
Introducing a Pole Concept for Nodule Growth in the Thyroid Gland: Taller-than-Wide Shape, Frequency, Location and Risk of Malignancy of Thyroid Nodules in an Area with Iodine Deficiency
Abstract
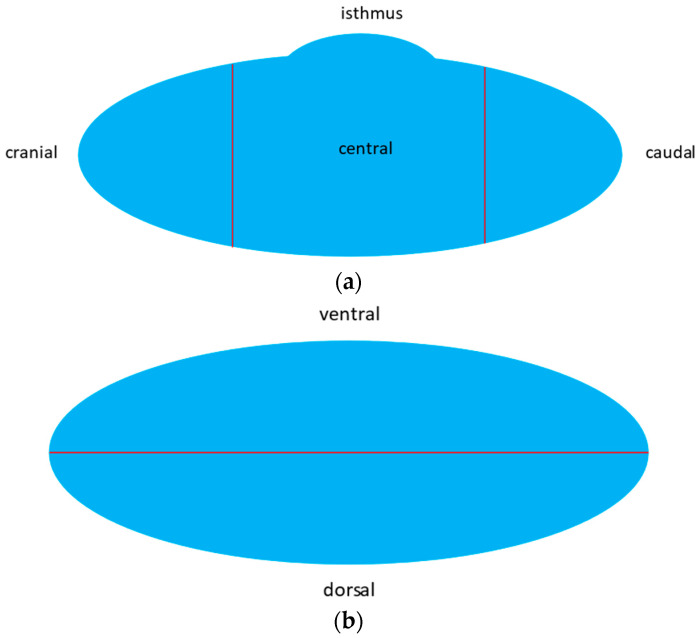
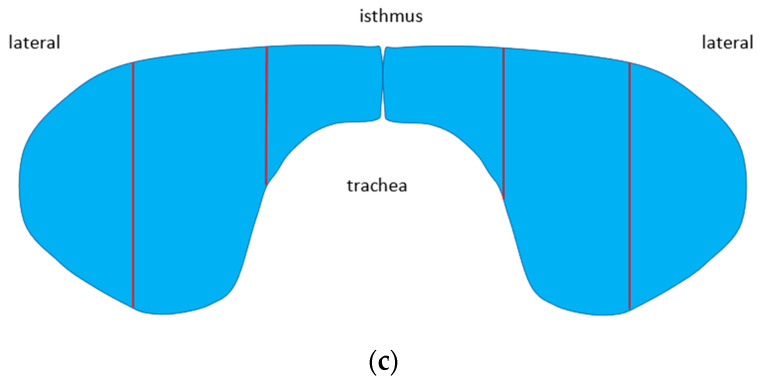
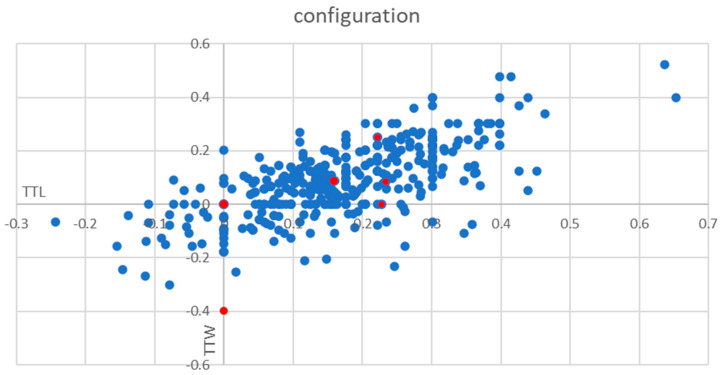
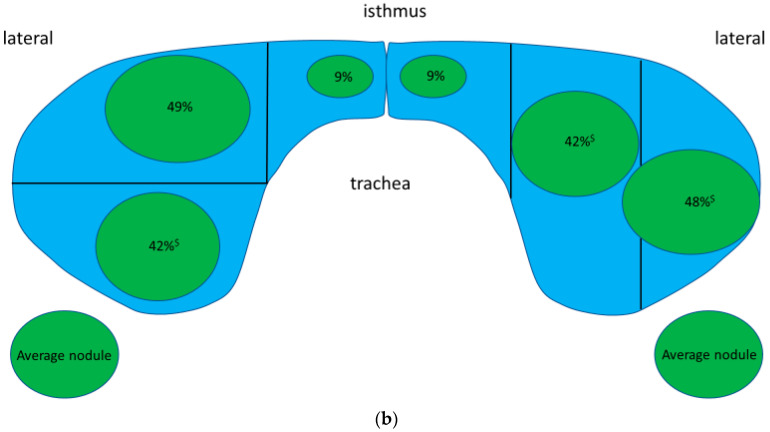
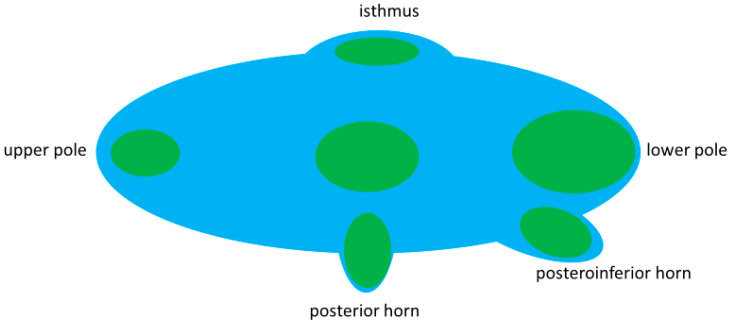
Purpose: (i) To examine the criterion taller-than-wide (TTW) for the sonographic assessment of thyroid nodules in areas of iodine deficiency in terms of frequency, anatomical distribution within the thyroid gland and risk of malignancy. (ii) To develop a model for nodule growth in the thyroid gland. Methods: German multicenter study consisting of two parts. In the prospective part, thyroid nodules were sonographically measured in all three dimensions, location within the thyroid gland and contact to a protrusion-like formation (horn) in the dorsal position of thyroid gland was noted. In addition, further sonographic features such as the composition, echogenity, margins and calcifications were investigated. All nodules from the prospective part were assessed for malignancy as part of clinical routine at the decision of the treating physician adhering to institutionally based algorithms. In the retrospective part, only nodules with fine needle aspiration and/or histology were included. The risk of malignancy in TTW nodules was determined by correlating them with cyotological and histological results. Results: Prospective part: out of 441 consecutively evaluated thyroid nodules, 6 were found to be malignant (1.4%, 95% CI 0.6-2.7%). Among the 74 TTW nodules (17%), 1 was malignant (1%, 95% CI 0-4%). TTW nodules were more often located in the dorsal half of the thyroid than non-TTW nodules (factor 2.3, p = 0.01, 95% CI 2.1-2.5) and more often located in close proximity to a horn than non-TTW nodules (factor 3.0, p = 0.01, 95% CI 2.4-3.8). Retrospective part: out of 1315 histologically and/or cytologically confirmed thyroid nodules, 163 TTW nodules were retrieved and retrospectively analyzed. A TTW nodule was 1.7 times more often benign when it was dorsal (95% CI 1.1-2.5) and 2.5 times more often benign when it was associated with a horn (95% CI 1.2-5.3). The overall probability of malignancy for TTW nodules was 38% (95% CI 30-46%) in this highly preselected patient group. Conclusion: TTW nodules are common in iodine deficient areas. They are often located in the dorsal half of the thyroid gland and are frequently associated with a dorsal protrusion-like formation (horn) of the thyroid. Obviously, the shape of benign nodules follows distinct anatomical preconditions within the thyroid gland. The frequency of TTW nodules and their predominant benignity can be explained by a pole concept of goiter growth. The difference between the low malignancy risk of TTW nodules found on a prospective basis and the high risk found retrospectively may be the result of a positive preselection in the latter.
Keywords: TIRADS; TTW nodules; Zuckerkandl’s tubercle; pole concept of goiter growth; posterior horn; posteroinferior horn; risk of malignancy; taller-than-wide.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Thyroid Imaging Reporting and Data Systems: Applicability of the "Taller than Wide" Criterium in Primary/Secondary Care Units and the Role of Thyroid Scintigraphy.J Clin Med. 2024 Jan 17;13(2):514. doi: 10.3390/jcm13020514. J Clin Med. 2024. PMID: 38256648 Free PMC article.
-
Thyroid Nodule Sphericity Metrics Discriminate Benign and Malignant Follicular and Oncocytic Neoplasms.Thyroid. 2025 Mar;35(3):291-297. doi: 10.1089/thy.2024.0670. Epub 2025 Feb 25. Thyroid. 2025. PMID: 39992747
-
Histopathological Analysis of Thyroid Nodules with Taller-Than-Wide Shape in Adults.Int J Gen Med. 2024 Nov 7;17:5123-5131. doi: 10.2147/IJGM.S473731. eCollection 2024. Int J Gen Med. 2024. PMID: 39534592 Free PMC article.
-
Risk Stratification of Thyroid Nodules: From Ultrasound Features to TIRADS.Cancers (Basel). 2022 Jan 30;14(3):717. doi: 10.3390/cancers14030717. Cancers (Basel). 2022. PMID: 35158985 Free PMC article. Review.
-
Usefulness of different ultrasound features of malignancy in predicting the type of thyroid lesions: a meta-analysis of prospective studies.Pol Arch Med Wewn. 2014;124(3):97-104. doi: 10.20452/pamw.2132. Epub 2014 Jan 28. Pol Arch Med Wewn. 2014. PMID: 24473342 Review.
Cited by
-
Thyroid Imaging Reporting and Data Systems: Applicability of the "Taller than Wide" Criterium in Primary/Secondary Care Units and the Role of Thyroid Scintigraphy.J Clin Med. 2024 Jan 17;13(2):514. doi: 10.3390/jcm13020514. J Clin Med. 2024. PMID: 38256648 Free PMC article.
References
-
- Schaffner M., Rochau U., Mühlberger N., Conrads-Frank A., Qerimi Rushaj V., Sroczynski G., Koukkou E., Thuesen B.H., Völzke H., Oberaigner W., et al. The economic impact of prevention, monitoring and treatment strategies for iodine deficiency disorders in Germany. Endocr. Connect. 2021;10:1–12. doi: 10.1530/EC-20-0384. - DOI - PMC - PubMed
-
- Seifert P., Schenke S., Zimny M., Stahl A., Grunert M., Klemenz B., Freesmeyer M., Kreissl M.C., Herrmann K., Görges R. Diagnostic Performance of Kwak, EU, ACR, and Korean TIRADS as Well as ATA Guidelines for the Ultrasound Risk Stratification of Non-Autonomously Functioning Thyroid Nodules in a Region with Long History of Iodine Deficiency: A German Multicenter Trial. Cancers. 2021;13:4467. doi: 10.3390/cancers13174467. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
